

Factors Influencing Depression Endpoints Research (FINDER): baseline results of Italian patients with depression
- PMID: 19480684
- PMCID: PMC2701433
- DOI: 10.1186/1744-859X-8-14
Factors Influencing Depression Endpoints Research (FINDER): baseline results of Italian patients with depression
Abstract
Background: Factors Influencing Depression Endpoints Research (FINDER) is a 6-month, prospective, observational study carried out in 12 European countries aimed at investigating health-related quality of life (HRQoL) in outpatients receiving pharmacological treatment for a first or new depressive episode. Baseline characteristics of patients enrolled in Italy are presented.
Methods: All treatment decisions were at the discretion of the investigator. Data were collected at baseline and after 3 and 6 months of treatment. Baseline evaluations included demographics, medical and psychiatric history, and medications used in the last 24 months and prescribed at enrollment. The Hospital Anxiety and Depression Scale (HADS), was adopted to evaluate depressive symptoms, while somatic and painful physical symptoms were assessed by using the Somatic Symptom Inventory (SSI) and a 0 to 100 mm visual analogue scale (VAS), HRQoL via 36-item Short Form Health Survey (SF-36), and the European Quality of Life 5-Dimensions (EQ-5D) instrument.
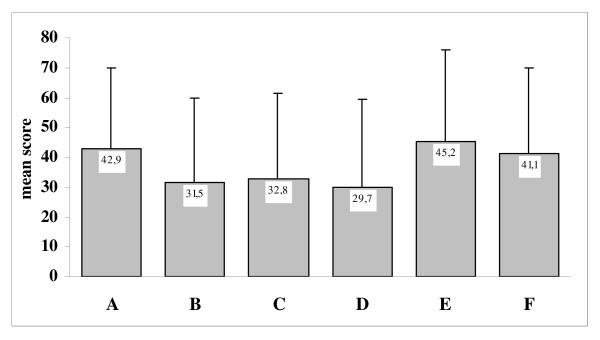
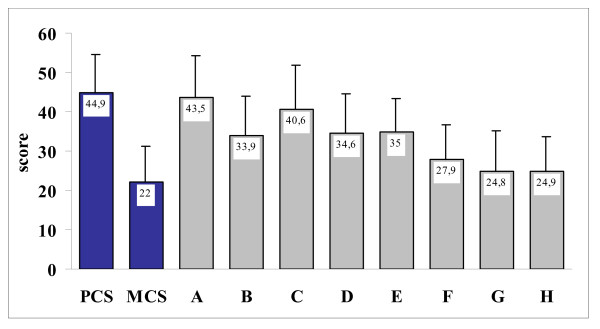
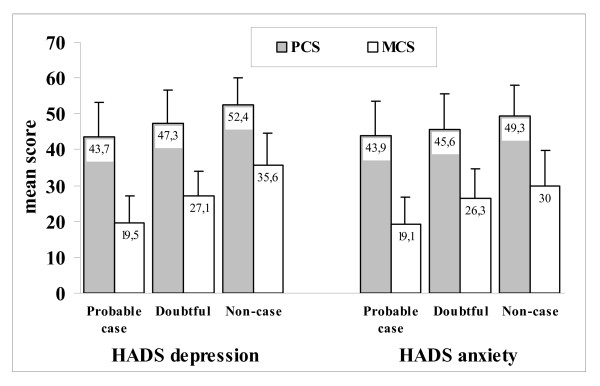
Results: A total of 513 patients were recruited across 38 sites. The mean +/- standard deviation (SD) age at first depressive episode was 38.7 +/- 15.9 years, the mean duration of depression 10.6 +/- 12.3 years. The most common psychiatric comorbidities in the previous 24 months were anxiety/panic (72.6%) and obsessive/compulsive disorders (13.4%), while 35.9% had functional somatic syndromes. Most patients (65.1%) reported pain from any cause. Monotherapy with selective serotonin reuptake inhibitors (SSRIs) and tricyclic antidepressants (TCAs) was prescribed at enrollment in 64.5% and 6.4% of the cases, respectively. The most commonly prescribed agents were sertraline (17.3%), escitalopram (16.2%), venlaflaxine (15.6%) and paroxetine (14.8%). The mean HADS subscores for depression and anxiety were 13.3 +/- 4.2 and 12.2 +/- 3.9, respectively; 76.4% of patients could be defined as being 'probable cases' for depression and 66.2% for anxiety. The mean total score of VAS-pain in the last week was 42.9 +/- 27.1, with highest scores reported in the 'interference of pain with daily activities' and in 'amount of time patient was awake and had pain'. From SF-36, the worst health status was found for role limitations due to emotional problem, mental health and social functioning. A mean score < 50 (that is, below the standardised population norm) was also found in all remaining domains. The SF-36 summary scores and EQ-5D (health status and VAS) were lower in patients with moderate/severe pain than in those with no or mild pain.
Conclusion: The baseline results of patients enrolled in the FINDER study in Italy show clinical and functional impairments, and poor HRQoL. The results obtained after 6 months of therapy will permit better understanding the effects of different variables on clinical outcomes and HRQoL.
Figures
References
-
- Simon GE, Von Korff M. Suicide mortality among patients treated for depression in an insured population. Am J Epidemiol. 1998;147:155–160. - PubMed
-
- Lecrubier Y. The burden of depression and anxiety in general medicine. J Clin Psychiatry. 2001;62:4–9. - PubMed
-
- Mueller TI, Leon AC, Keller MB, Solomon DA, Endicott J, Coryell W, Warshaw M, Maser JD. Recurrence after recovery from major depressive disorder during 15 years of observational follow-up. Am J Psychiatry. 1999;156:1000–1006. - PubMed
-
- Thase ME. Achieving remission and managing relapse in depression. J Clin Psychiatry. 2003;64:3–7. - PubMed
LinkOut - more resources
Full Text Sources
