

Achieved anticoagulation vs prosthesis selection for mitral mechanical valve replacement: a population-based outcome study
- PMID: 19482955
- PMCID: PMC2789923
- DOI: 10.1378/chest.08-1233
Achieved anticoagulation vs prosthesis selection for mitral mechanical valve replacement: a population-based outcome study
Abstract
Background: Thromboembolic events (TEs) are frequent after mechanical mitral valve replacement (MVR), but their association to anticoagulation quality is unclear and has never been studied in a population-based setting with patients who have a complete anticoagulation record.
Methods: We compiled a complete record of all residents of Olmsted County, MN, who underwent mechanical MVR between 1981 and 2004, for all TE, bleeding episodes, and international normalized ratios (INRs) measured from prosthesis implantation.
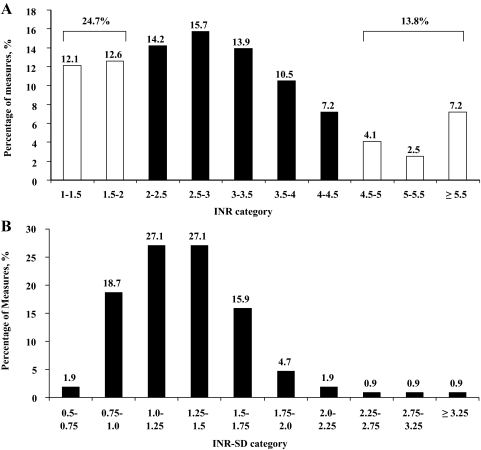
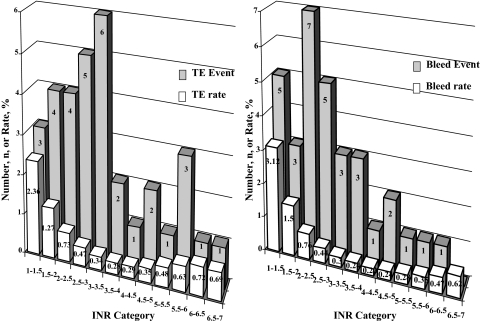
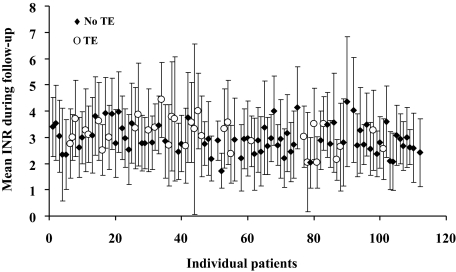
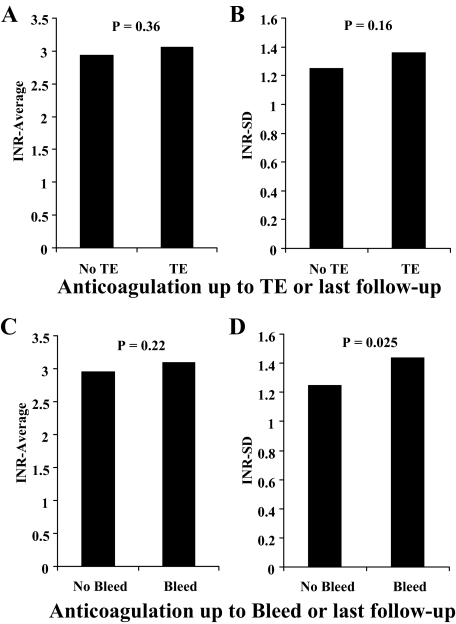
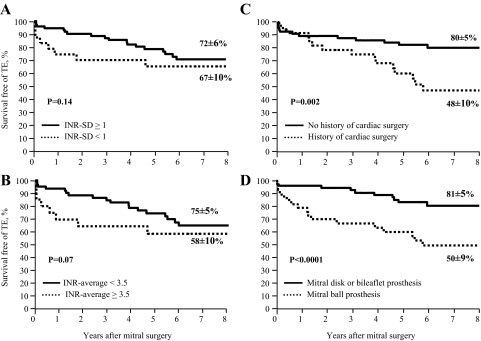
Results: In the 112 residents (mean [+/- SD] age, 57 +/- 16 years; 60% female residents) who underwent mechanical MVR, 19,647 INR samples were obtained. While INR averaged 3.02 +/- 0.57, almost 40% of INRs were < 2 or > 4.5. Thirty-four TEs and 28 bleeding episodes occurred during a mean duration of 8.2 +/- 6.1 years of follow-up. There was no trend of association of INR (average, SD, growth variance rate, or intensity-specific incidence of events) with TE. Previous cardiac surgery (p = 0.014) and ball prosthesis (hazard ratio [HR], 2.92; 95% CI, 1.43 to 5.94; p = 0.003) independently determined TE. With MVR using a ball prosthesis, despite higher anticoagulation intensity (p = 0.002), the 8-year rate of freedom from TE was considerably lower (50 +/- 9% vs 81 +/- 5%, respectively; p < 0.0001). Compared with expected stroke rates in the population, stroke risk was elevated with non-ball prosthesis MVR (HR 2.6; 95% CI, 1.3 to 5.2; p = 0.007) but was considerable with ball prosthesis MVR (HR 11.7; 95% CI, 7.5 to 18.4; p < 0.0001). INR variability (SD) was higher with a higher mean INR value (p < 0.0001). INR variability (HR 2.485; 95% CI, 1.11 to 5.55; p = 0.027) and cancer history (p < 0.0001) independently determined bleeding rates.
Conclusion: This population-based comprehensive study of anticoagulation and TE post-MVR shows that, in these closely anticoagulated patients, anticoagulation intensity was highly variable and not associated with TE incidence post-MVR. Higher anticoagulation intensity is linked to higher variability and, thus, to bleeding. The MVR-ball prosthesis design is associated with higher TE rates notwithstanding higher anticoagulation intensity, and its use should be retired worldwide.
Figures
Comment in
-
Balancing thromboembolism and bleeding risks: insights from anticoagulation for prosthetic heart valves.Chest. 2009 Dec;136(6):1451-1452. doi: 10.1378/chest.09-1187. Chest. 2009. PMID: 19995760 No abstract available.
Similar articles
-
Analysis of Anticoagulation Therapy and Anticoagulation-Related Outcomes Among Asian Patients After Mechanical Valve Replacement.JAMA Netw Open. 2022 Feb 1;5(2):e2146026. doi: 10.1001/jamanetworkopen.2021.46026. JAMA Netw Open. 2022. PMID: 35103794 Free PMC article.
-
Incidence and risk factors for thromboembolism and major bleeding in patients with mechanical valve prosthesis: A nationwide population-based study.Am Heart J. 2016 Nov;181:1-9. doi: 10.1016/j.ahj.2016.06.026. Epub 2016 Aug 11. Am Heart J. 2016. PMID: 27823679
-
Anticoagulation therapy and related outcomes among Asian patients after bioprosthetic valve replacement.BMC Cardiovasc Disord. 2025 May 28;25(1):413. doi: 10.1186/s12872-025-04837-y. BMC Cardiovasc Disord. 2025. PMID: 40437381 Free PMC article.
-
[Anticoagulation of valvular prostheses].Ann Cardiol Angeiol (Paris). 2003 Nov;52(5):290-6. doi: 10.1016/s0003-3928(03)00097-0. Ann Cardiol Angeiol (Paris). 2003. PMID: 14714342 Review. French.
-
Safety and Use of Anticoagulation After Aortic Valve Replacement With Bioprostheses: A Meta-Analysis.Circ Cardiovasc Qual Outcomes. 2016 May;9(3):294-302. doi: 10.1161/CIRCOUTCOMES.115.002696. Epub 2016 May 10. Circ Cardiovasc Qual Outcomes. 2016. PMID: 27166205 Free PMC article. Review.
Cited by
-
Management of therapeutic anticoagulation in patients with intracerebral haemorrhage and mechanical heart valves.Eur Heart J. 2018 May 14;39(19):1709-1723. doi: 10.1093/eurheartj/ehy056. Eur Heart J. 2018. PMID: 29529259 Free PMC article.
-
Outcomes related to anticoagulation management for mechanical valve replacements.J Thorac Dis. 2021 May;13(5):2874-2884. doi: 10.21037/jtd-20-2562. J Thorac Dis. 2021. PMID: 34164179 Free PMC article.
-
Clinical mid-term outcomes of the Chinese-made CL-V bileaflet mechanical heart valve in Chinese patients.J Thorac Dis. 2021 Jan;13(1):10-17. doi: 10.21037/jtd-20-2644. J Thorac Dis. 2021. PMID: 33569180 Free PMC article.
-
Thrombotic dysfunction of mechanical mitral valve.Herz. 2014 Aug;39(5):601-2. doi: 10.1007/s00059-013-3837-8. Epub 2013 Jun 9. Herz. 2014. PMID: 23749196 No abstract available.
-
Effect of Quinolones Versus Cefixime on International Normalized Ratio Levels After Valve Replacement Surgery with Warfarin Therapy.Medicina (Kaunas). 2019 Sep 26;55(10):644. doi: 10.3390/medicina55100644. Medicina (Kaunas). 2019. PMID: 31561580 Free PMC article.
References
-
- Nkomo VT, Gardin JM, Skelton TN, et al. Burden of valvular heart diseases: a population-based study. Lancet. 2006;368:1005–1011. - PubMed
-
- Bonow RO, Carabello BA, Chatterjee K, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing Committee to Revise the 1998 guidelines for the management of patients with valvular heart disease) developed in collaboration with the Society of Cardiovascular Anesthesiologists endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2006;48:e1–e148. - PubMed
-
- Hering D, Piper C, Bergemann R, et al. Thromboembolic and bleeding complications following St. Jude Medical valve replacement: results of the German experience with low-intensity anticoagulation study. Chest. 2005;127:53–59. - PubMed
-
- Kuntze CE, Blackstone EH, Ebels T. Thromboembolism and mechanical heart valves: a randomized study revisited. Ann Thorac Surg. 1998;66:101–107. - PubMed
-
- Grunkemeier GL, Wu Y. “Our complication rates are lower than theirs”: statistical critique of heart valve comparisons. J Thorac Cardiovasc Surg. 2003;125:290–300. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
