

Integrating health status and survival data: the palliative effect of lung volume reduction surgery
- PMID: 19483114
- PMCID: PMC2724716
- DOI: 10.1164/rccm.200809-1383OC
Integrating health status and survival data: the palliative effect of lung volume reduction surgery
Abstract
Rationale: In studies that address health-related quality of life (QoL) and survival, subjects who die are usually censored from QoL assessments. This practice tends to inflate the apparent benefits of interventions with a high risk of mortality. Assessing a composite QoL-death outcome is a potential solution to this problem.
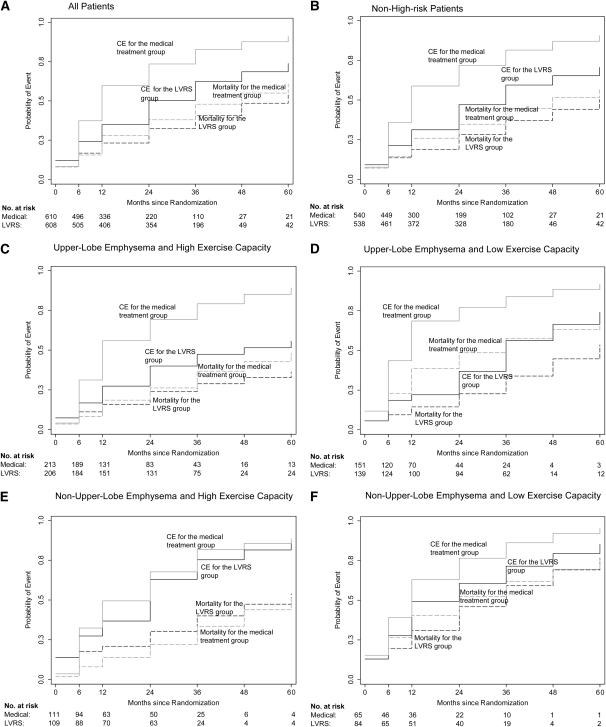
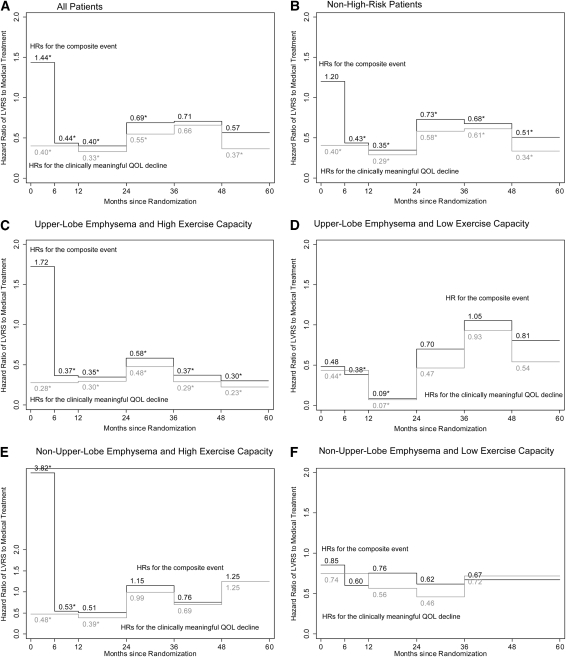
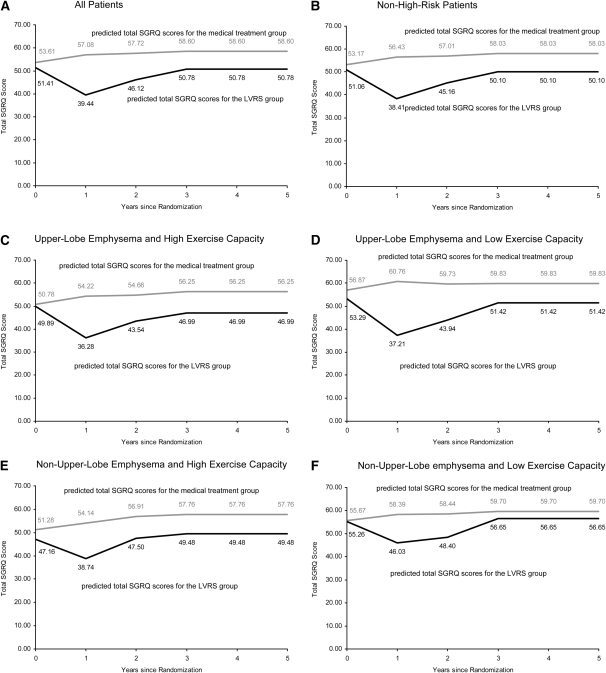
Objectives: To determine the effect of lung volume reduction surgery (LVRS) on a composite endpoint consisting of the occurrence of death or a clinically meaningful decline in QoL defined as an increase of at least eight points in the St. George's Respiratory Questionnaire total score from the National Emphysema Treatment Trial.
Methods: In patients with chronic obstructive pulmonary disease and emphysema randomized to receive medical treatment (n = 610) or LVRS (n = 608), we analyzed the survival to the composite endpoint, the hazard functions and constructed prediction models of the slope of QoL decline.
Measurements and main results: The time to the composite endpoint was longer in the LVRS group (2 years) than the medical treatment group (1 year) (P < 0.0001). It was even longer in the subsets of patients undergoing LVRS without a high risk for perioperative death and with upper-lobe-predominant emphysema. The hazard for the composite event significantly favored the LVRS group, although it was most significant in patients with predominantly upper-lobe emphysema. The beneficial impact of LVRS on QoL decline was most significant during the 2 years after LVRS.
Conclusions: LVRS has a significant effect on the composite QoL-survival endpoint tested, indicating its meaningful palliative role, particularly in patients with upper-lobe-predominant emphysema.
Figures
References
-
- Yusen RD, Littenberg B. Integrating survival and quality of life data in clinical trials of lung disease: the case of lung volume reduction surgery. Chest 2005;127:1094–1096. - PubMed
-
- Fishman A, Martinez F, Naunheim K, Piantadosi S, Wise R, Ries A, Weinmann G, Wood DE. A randomized trial comparing lung-volume-reduction surgery with medical therapy for severe emphysema. N Engl J Med 2003;348:2059–2073. - PubMed
-
- Naunheim KS, Wood DE, Mohsenifar Z, Sternberg AL, Criner GJ, DeCamp MM, Deschamps CC, Martinez FJ, Sciurba FC, Tonascia J, et al. Long-term follow-up of patients receiving lung-volume-reduction surgery versus medical therapy for severe emphysema by the national emphysema treatment trial research group. Ann Thorac Surg 2006;82:431–443. - PubMed
-
- Benzo R, Kaplan MR, Martinez F, Wise R, Make B, Criner G, Reilly J, Fishman A, Luketich J, Sciurba F. Effect of lung volume reduction surgery on the decline of health related quality of life [abstract]. Am J Respir Crit Care Med 2007;175:A175.
-
- The National Emphysema Treatment Trial Research Group. Rationale and design of the national emphysema treatment trial (NETT): a prospective randomized trial of lung volume reduction surgery. J Thorac Cardiovasc Surg 1999;118:518–528. - PubMed
Publication types
MeSH terms
Grants and funding
- N01HR76113/HR/NHLBI NIH HHS/United States
- N01HR76104/HR/NHLBI NIH HHS/United States
- N01HR76105/HR/NHLBI NIH HHS/United States
- K23 CA106544/CA/NCI NIH HHS/United States
- N01HR76110/HR/NHLBI NIH HHS/United States
- N01HR76119/HR/NHLBI NIH HHS/United States
- N01HR76108/HR/NHLBI NIH HHS/United States
- N01HR76106/HR/NHLBI NIH HHS/United States
- N01HR76109/HR/NHLBI NIH HHS/United States
- N01HR76116/HR/NHLBI NIH HHS/United States
- 1K23CA106544/CA/NCI NIH HHS/United States
- N01HR76112/HR/NHLBI NIH HHS/United States
- N01HR76101/HR/NHLBI NIH HHS/United States
- N01HR76107/HR/NHLBI NIH HHS/United States
- N01HR76102/HR/NHLBI NIH HHS/United States
- N01HR76118/HR/NHLBI NIH HHS/United States
- N01HR76115/HR/NHLBI NIH HHS/United States
- N01HR76111/HR/NHLBI NIH HHS/United States
- N01HR76114/HR/NHLBI NIH HHS/United States
- N01HR76103/HR/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
