

Risk of colorectal cancer seven years after flexible sigmoidoscopy screening: randomised controlled trial
- PMID: 19483252
- PMCID: PMC2688666
- DOI: 10.1136/bmj.b1846
Risk of colorectal cancer seven years after flexible sigmoidoscopy screening: randomised controlled trial
Abstract
Objective: To determine the risk of colorectal cancer after screening with flexible sigmoidoscopy.
Design: Randomised controlled trial.
Setting: Population based screening in two areas in Norway-city of Oslo and Telemark county (urban and mixed urban and rural populations).
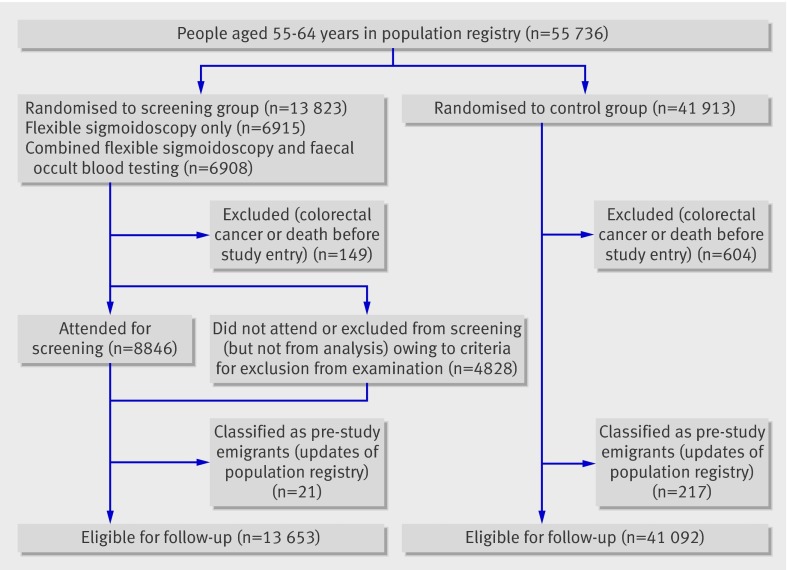
Participants: 55 736 men and women aged 55-64 years.
Intervention: Once only flexible sigmoidoscopy screening with or without a single round of faecal occult blood testing (n=13 823) compared with no screening (n=41 913).
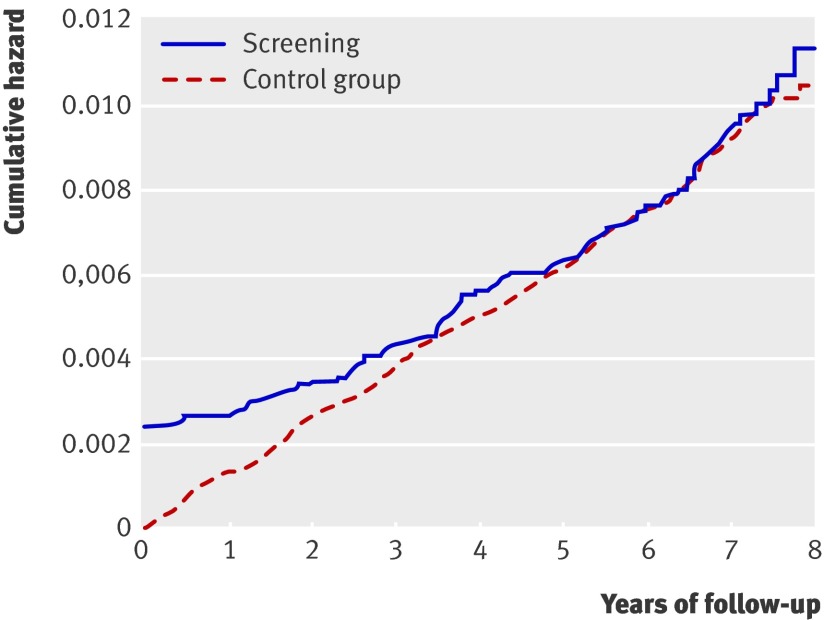
Main outcome measures: Planned end points were cumulative incidence and mortality of colorectal cancer after 5, 10, and 15 years. This first report from the study presents cumulative incidence after 7 years of follow-up and hazard ratio for mortality after 6 years.
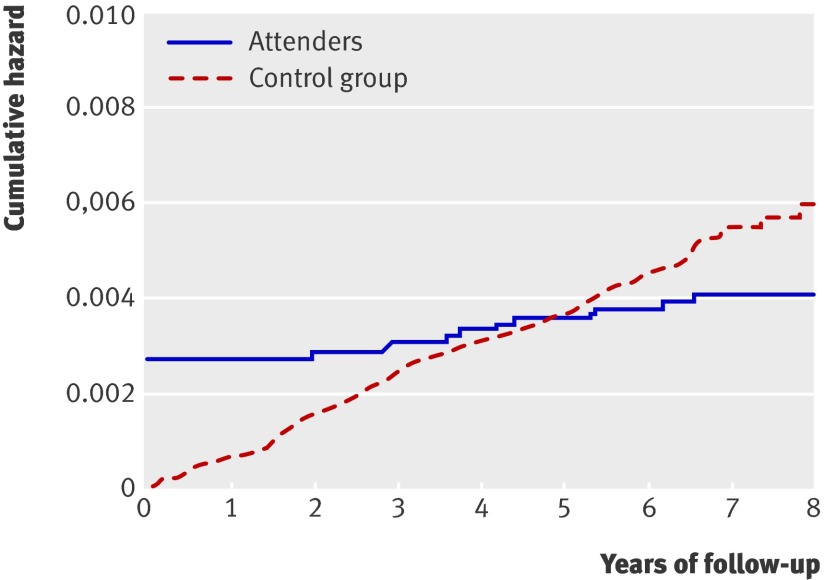
Results: No difference was found in the 7 year cumulative incidence of colorectal cancer between the screening and control groups (134.5 v 131.9 cases per 100 000 person years). In intention to screen analysis, a trend towards reduced colorectal cancer mortality was found (hazard ratio 0.73, 95% confidence interval 0.47 to 1.13, P=0.16). For attenders compared with controls, a statistically significant reduction in mortality was apparent for both total colorectal cancer (hazard ratio 0.41, 0.21 to 0.82, P=0.011) and rectosigmoidal cancer (0.24, 0.08 to 0.76, P=0.016).
Conclusions: A reduction in incidence of colorectal cancer with flexible sigmoidoscopy screening could not be shown after 7 years' follow-up. Mortality from colorectal cancer was not significantly reduced in the screening group but seemed to be lower for attenders, with a reduction of 59% for any location of colorectal cancer and 76% for rectosigmoidal cancer in per protocol analysis, an analysis prone to selection bias.
Trial registration: Clinical trials NCT00119912.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Sigmoidoscopy screening for colorectal cancer.BMJ. 2009 May 29;338:b2084. doi: 10.1136/bmj.b2084. BMJ. 2009. PMID: 19483253 No abstract available.
-
Colorectal cancer. Limitations of trial.BMJ. 2009 Jun 23;338:b2531. doi: 10.1136/bmj.b2531. BMJ. 2009. PMID: 19549661 No abstract available.
-
Does flexible sigmoidoscopy reduce colorectal cancer incidence and mortality?Gastroenterology. 2009 Oct;137(4):1529-31. doi: 10.1053/j.gastro.2009.08.022. Epub 2009 Aug 28. Gastroenterology. 2009. PMID: 19717128 No abstract available.
-
Once-only flexible sigmoidoscopy screening for colorectal cancer may not reduce colorectal cancer incidence or mortality.Evid Based Med. 2009 Dec;14(6):171. doi: 10.1136/ebm.14.6.171. Evid Based Med. 2009. PMID: 19949173 No abstract available.
References
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin 2005;55:74-108. - PubMed
-
- Rex DK, Johnson DA, Lieberman DA, Burt RW, Sonnenberg A. Colorectal cancer prevention 2000: screening recommendations of the American College of Gastroenterology. Am J Gastroenterol 2000;95:868-77. - PubMed
-
- Regula J, Rupinski M, Kraszewska E, Polkowski M, Pachlewski J, Orlowska J, et al. Colonoscopy in colorectal-cancer screening for detection of advanced neoplasia. N Engl J Med 2006;355:1863-72. - PubMed
-
- Rozen P, Winawer SJ. Report of the OMED colorectal cancer screening committee meeting, New Orleans, 2004—in collaboration with the IDCA. Eur J Cancer Prev 2004;13:461-4. - PubMed
-
- Winawer SJ, Zauber AG, Ho MN, O’Brian MJ, Gottlieb LS, Sternberg SS, et al. Prevention of colorectal cancer by colonoscopic polypectomy. N Engl J Med 1993;329:1977-81. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical