

Cognitive-behavioral therapy versus usual clinical care for youth depression: an initial test of transportability to community clinics and clinicians
- PMID: 19485581
- PMCID: PMC3010274
- DOI: 10.1037/a0013877
Cognitive-behavioral therapy versus usual clinical care for youth depression: an initial test of transportability to community clinics and clinicians
Abstract
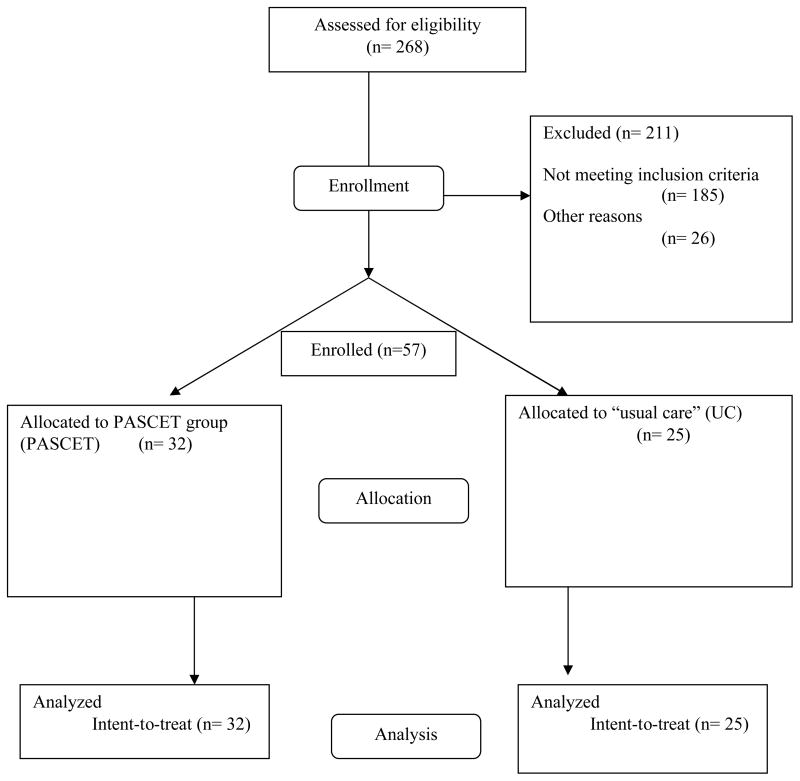
Community clinic therapists were randomized to (a) brief training and supervision in cognitive-behavioral therapy (CBT) for youth depression or (b) usual care (UC). The therapists treated 57 youths (56% girls), ages 8-15, of whom 33% were Caucasian, 26% were African American, and 26% were Latino/Latina. Most youths were from low-income families and all had Diagnostic and Statistical Manual of Mental Disorders (4th ed.; American Psychiatric Association, 1994) depressive disorders (plus multiple comorbidities). All youths were randomized to CBT or UC and treated until normal termination. Session coding showed more use of CBT by CBT therapists and more psychodynamic and family approaches by UC therapists. At posttreatment, depression symptom measures were at subclinical levels, and 75% of youths had no remaining depressive disorder, but CBT and UC groups did not differ on these outcomes. However, compared with UC, CBT was (a) briefer (24 vs. 39 weeks), (b) superior in parent-rated therapeutic alliance, (c) less likely to require additional services (including all psychotropics combined and depression medication in particular), and (d) less costly. The findings showed advantages for CBT in parent engagement, reduced use of medication and other services, overall cost, and possibly speed of improvement--a hypothesis that warrants testing in future research.
Copyright 2009 APA
References
-
- Achenbach TM. Manual for the child behavior checklists/4–18 and 1991 profile. Burlington, VT: University of Vermont; 1991.
-
- Achenbach TM. Manual for the Child Behavior Checklist/4–18 and 1991 Profile. Burlington, VT: University of Vermont Department of Psychiatry; 1991a.
-
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4. Washington, DC: American Psychiatric Association; 1994. rev.
-
- Birmaher B, Brent DA, Benson RS. Summary of the practice parameters for the assessment and treatment of children and adolescents with depressive disorders. American Academy of Child and Adolescent Psychiatry, Work group on quality issues. Journal of the American Academy of Child and Adolescent Psychiatry. 1998;37:1234–1238. - PubMed
-
- Birmaher B, Brent DA, Kolko D, Baugher M, Bridge J, Holder D, Iyengar S, Uloa RE. Clinical outcome after short-term psychotherapy for adolescents with major depressive disorder. Archives of General Psychiatry. 2000;57:29–36. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
