

Diagnostic challenges of early Lyme disease: lessons from a community case series
- PMID: 19486523
- PMCID: PMC2698836
- DOI: 10.1186/1471-2334-9-79
Diagnostic challenges of early Lyme disease: lessons from a community case series
Abstract
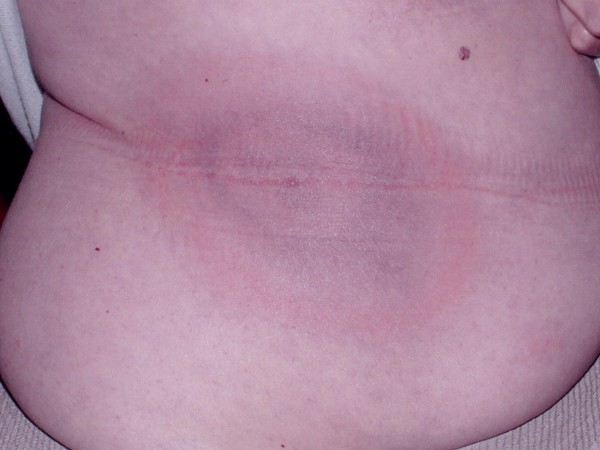
Background: Lyme disease, the most common vector-borne infection in North America, is increasingly reported. When the characteristic rash, erythema migrans, is not recognized and treated, delayed manifestations of disseminated infection may occur. The accuracy of diagnosis and treatment of early Lyme disease in the community is unknown.
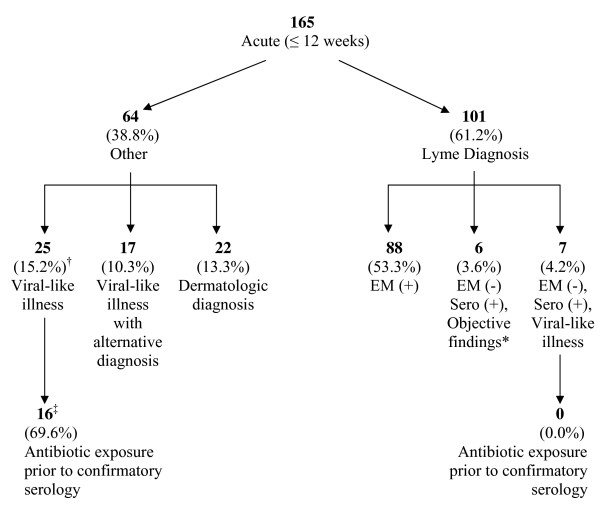
Methods: A retrospective, consecutive case series of 165 patients presenting for possible early Lyme disease between August 1, 2002 and August 1, 2007 to a community-based Lyme referral practice in Maryland. All patients had acute symptoms of less than or equal to 12 weeks duration. Patients were categorized according to the Centers for Disease Control and Prevention criteria and data were collected on presenting history, physical findings, laboratory serology, prior diagnoses and prior treatments.
Results: The majority (61%) of patients in this case series were diagnosed with early Lyme disease. Of those diagnosed with early Lyme disease, 13% did not present with erythema migrans; of those not presenting with a rash, 54% had been previously misdiagnosed. Among those with a rash, the diagnosis of erythema migrans was initially missed in 23% of patients whose rash was subsequently confirmed. Of all patients previously misdiagnosed, 41% had received initial antibiotics likely to be ineffective against Lyme disease.
Conclusion: For community physicians practicing in high-risk geographic areas, the diagnosis of Lyme disease remains a challenge. Failure to recognize erythema migrans or alternatively, viral-like presentations without a rash, can lead to missed or delayed diagnosis of Lyme disease, ineffective antibiotic treatment, and the potential for late manifestations.
Figures




Similar articles
-
Antibiotic therapy for Lyme disease in Maryland.Public Health Rep. 1994 Nov-Dec;109(6):745-9. Public Health Rep. 1994. PMID: 7800782 Free PMC article.
-
Maryland physicians' survey on Lyme disease.Md Med J. 1994 May;43(5):447-50. Md Med J. 1994. PMID: 8052097
-
Not All Erythema Migrans Lesions Are Lyme Disease.Am J Med. 2017 Feb;130(2):231-233. doi: 10.1016/j.amjmed.2016.08.020. Epub 2016 Sep 6. Am J Med. 2017. PMID: 27612442
-
Physical Therapist Recognition and Referral of Individuals With Suspected Lyme Disease.Phys Ther. 2021 Aug 1;101(8):pzab128. doi: 10.1093/ptj/pzab128. Phys Ther. 2021. PMID: 34003263 Free PMC article. Review.
-
Lyme disease.J Am Acad Nurse Pract. 2001 May;13(5):223-6; quiz 227-8. doi: 10.1111/j.1745-7599.2001.tb00024.x. J Am Acad Nurse Pract. 2001. PMID: 11930473 Review.
Cited by
-
Probable late lyme disease: a variant manifestation of untreated Borrelia burgdorferi infection.BMC Infect Dis. 2012 Aug 1;12:173. doi: 10.1186/1471-2334-12-173. BMC Infect Dis. 2012. PMID: 22853630 Free PMC article.
-
Geographical Distribution of Borrelia burgdorferi sensu lato in Ticks Collected from Wild Rodents in the Republic of Korea.Pathogens. 2020 Oct 22;9(11):866. doi: 10.3390/pathogens9110866. Pathogens. 2020. PMID: 33105824 Free PMC article.
-
The Emerging Role of Microbial Biofilm in Lyme Neuroborreliosis.Front Neurol. 2018 Dec 3;9:1048. doi: 10.3389/fneur.2018.01048. eCollection 2018. Front Neurol. 2018. PMID: 30559713 Free PMC article. Review.
-
Atypical Case of Lyme Neuroborreliosis With Hyponatremia.Cureus. 2022 Apr 23;14(4):e24413. doi: 10.7759/cureus.24413. eCollection 2022 Apr. Cureus. 2022. PMID: 35619853 Free PMC article.
-
The Clinical, Symptom, and Quality-of-Life Characterization of a Well-Defined Group of Patients with Posttreatment Lyme Disease Syndrome.Front Med (Lausanne). 2017 Dec 14;4:224. doi: 10.3389/fmed.2017.00224. eCollection 2017. Front Med (Lausanne). 2017. PMID: 29312942 Free PMC article.
References
-
- Bacon RM, Kugeler KJ, Mead PS. Centers for Disease Control and Prevention. Surveillance for Lyme disease – United States, 1992–2006. MMWR Surveill Summ. 2008;57:1–9. - PubMed
-
- Meek JI, Roberts CL, Smith EV Jr, Cartter ML. Underreporting of Lyme disease by Connecticut physicians, 1992. J Public Health Manage Pract. 1996;2:61–5. - PubMed
-
- Coyle BS, Strickland GT, Liang YY, Pena C, McCarter R, Israel E. The public health impact of Lyme disease in Maryland. J Infect Dis. 1996;173:1260–2. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
