

Kidney function estimated from serum creatinine and cystatin C and peripheral arterial disease in NHANES 1999-2002
- PMID: 19487236
- PMCID: PMC2719699
- DOI: 10.1093/eurheartj/ehp195
Kidney function estimated from serum creatinine and cystatin C and peripheral arterial disease in NHANES 1999-2002
Abstract
Aims: Serum cystatin C, a novel marker of kidney function, is reported to be superior to serum creatinine as a risk factor for atherosclerotic disease, but associations may vary across vascular beds.
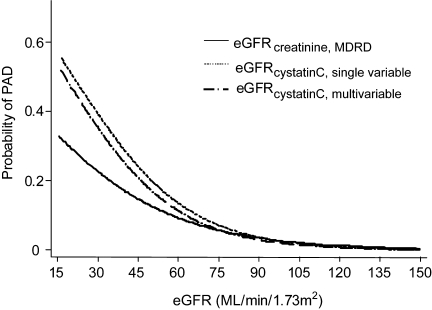
Methods and results: A cross-sectional study of chronic kidney disease (CKD) and peripheral arterial disease (PAD) in 3089 adult participants aged 40+ from the 1999-2002 National Health and Nutrition Examination Survey (NHANES). Kidney function, assessed by estimated glomerular filtration rate (eGFR), was determined from serum creatinine and cystatin C using established equations. Peripheral arterial disease defined by an ankle brachial index <0.90. Glomerular filtration rate estimated using cystatin C was more strongly associated with PAD compared with eGFR using serum creatinine before and after multivariable adjustment. Further, after adjustment for cystatin C, kidney function based on serum creatinine was no longer significantly associated with PAD. However, cystatin C remained significantly associated with PAD even after adjustment for GFR estimated by serum creatinine. Compared with optimal kidney function (eGFR(serum creatinine) >or=60, eGFR(cystatin C) >90), the odds ratio for PAD was 3.11 (95% confidence interval 1.26-7.64) for preclinical CKD (eGFR(serum creatinine) >or=60, eGFR(cystatin C) <76.7) and 5.07 (3.01-8.52) for 'confirmed' CKD (eGFR(serum creatinine) <60, eGFR(cystatin C) <60).
Conclusion: Chronic kidney disease was strongly and independently associated with PAD. Cystatin C was a more potent marker of lower extremity PAD when compared with the serum creatinine equation currently used in clinical practice. Our results suggest that cystatin C may have clinical utility when combined with serum creatinine in evaluation of individuals who may have PAD.
Figures
References
-
- Sarnak MJ, Levey AS, Schoolwerth AC, Coresh J, Culleton B, Hamm LL, McCullough PA, Kasiske BL, Kelepouris E, Klag MJ, Parfrey P, Pfeffer M, Raij L, Spinosa DJ, Wilson PW. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Hypertension. 2003;42:1050–1065. - PubMed
-
- Weiner DE, Tighiouart H, Amin MG, Stark PC, Macleod B, Griffith JL, Salem DN, Levey AS, Sarnak MJ. Chronic kidney disease as a risk factor for cardiovascular disease and all-cause mortality: a pooled analysis of community-based studies. J Am Soc Nephrol. 2004;15:1307–1315. - PubMed
-
- Landray MJ, Thambyrajah J, McGlynn FJ, Jones HJ, Baigent C, Kendall MJ, Townend JN, Wheeler DC. Epidemiological evaluation of known and suspected cardiovascular risk factors in chronic renal impairment. Am J Kidney Dis. 2001;38:537–546. - PubMed
-
- O'Hare A, Johansen K. Lower-extremity peripheral arterial disease among patients with end-stage renal disease. J Am Soc Nephrol. 2001;12:2838–2847. - PubMed
-
- Luscher TF, Creager MA, Beckman JA, Cosentino F. Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: part II. Circulation. 2003;108:1655–1661. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
