

Review
doi: 10.1172/JCI38937.
Epub 2009 Jun 1.
Pathogenesis of holoprosencephaly
Affiliations
- PMID: 19487816
- PMCID: PMC2689134
- DOI: 10.1172/JCI38937
Item in Clipboard
Review
Pathogenesis of holoprosencephaly
J Clin Invest.
2009 Jun.
Abstract
Holoprosencephaly (HPE), the most common human forebrain malformation, occurs in 1 in 250 fetuses and 1 in 16,000 live births. HPE is etiologically heterogeneous, and its pathology is variable. Several mouse models of HPE have been generated, and some of the molecular causes of different forms of HPE and the mechanisms underlying its variable pathology have been revealed by these models. Herein, we summarize the current knowledge on the genetic alterations that cause HPE and discuss some important questions about this disease that remain to be answered.
Figures
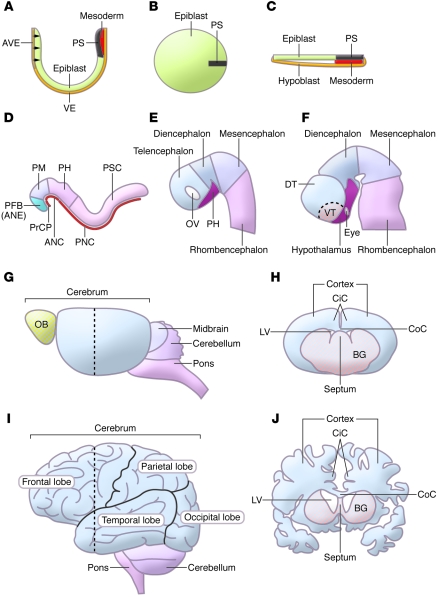
(A–C) At early primitive-streak stage,
epiblast cells ingress through the primitive streak (PS) to form the mesoderm.
Medial sagittal section of E6.5 mouse (A) and Carnegie Stage 7 (CS7)
human (B) embryos with anterior to the left. (C) Dorsal
view of a CS7 human embryo. AVE, anterior visceral endoderm; VE, visceral
endoderm. (D) At early somite stage (E8.5 for mouse; CS10 for human),
the neural ectoderm has been specified into different regions along the
anterior-posterior axis and the axial mesoderm is underlying the midline of the
neural ectoderm. ANC, anterior notochord; PFB, prospective forebrain (or ANE); PH,
prospective hindbrain; PM, prospective midbrain; PNC, posterior notochord; PSC,
prospective spinal chord. (E) Neural tube closure occurs at around
the 15-somite stage (E9.0 for mouse; CS11 for human). The forebrain gets further
regionalized into telencephalon, diencephalon, and prospective hypothalamus (PH).
OV, optic vesicle. (F) Approximately at E10.5 in the mouse or at CS14
in human embryos, the expanding telencephalon bifurcates dorsally to form the two
hemispheres and gets patterned into dorsal telencephalon (DT) and ventral
telencephalon (VT). (G and I) Lateral views of adult
mouse (G) and human brain (I). OB, olfactory bulb. Black
dashed lines in G and I indicate the location of coronal
sections shown in H and J. (H and
J) Coronal sections of adult mouse (H) and human brain
(J). BG, basal ganglia; CiC, cingulate cortex; CoC, corpus
callosum; LV, lateral ventricle.
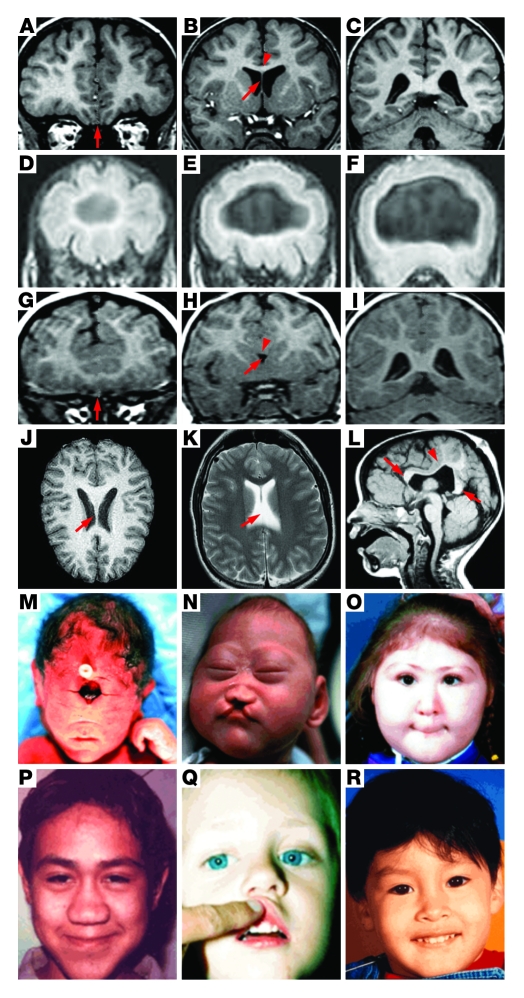
(A–I) Coronal images of control and HPE
brains from anterior (A, D, and G) to
posterior (C, F, and I).
(A–C) In the control brain, the two
hemispheres are separated completely (arrow in A) and the septum
(arrow in B) and the corpus callosum (arrowhead in B)
are present. (D–F) In alobar HPE, a single
cerebral ventricle is present and the interhemispheric fissure is completely
absent. (G–I) In semilobar HPE, the two
hemispheres are incompletely separated (arrow in G) and the septum
and corpus callosum are absent (arrow and arrowhead in H,
respectively). (J and K) Horizontal images of control
(J) and lobar HPE (K). The septum is present in the
control brain (arrow in J); however, it is partially absent in the
lobar HPE brain (arrow in K). (L) Sagittal image of a
MIH brain. The genu and splenium of the corpus callosum are present (arrows in
L); however, the corpus callosum is absent at the region lacking
the interhemispheric fissure (arrowhead in L).
(M–O) Craniofacial defects associated
with HPE. (M) Alobar HPE with cyclopia and proboscis.
(N) Semilobar HPE with microcephaly and cleft lip and palate.
(O) Semilobar HPE with ocular hypotelorism and midface hypoplasia.
(P and Q) Microforms of HPE. (P) Absence
of nasal bones and cartilage with a narrow nasal bridge. (Q) Single
central maxillary incisor. (R) MIH patient with normal facial
appearance. A–C and
G–I are reprinted with permission from
Cerebral cortex (17);
D–F are reprinted with permission from
American Journal of Medical Genetics (18); J is reprinted with permission from Brain
Maps (111); K is reprinted
with permission from MedPix (112);
L is reprinted with permission from American Journal of
Neuroradiology (23);
M and O are reprinted with permission from Human
Molecular Genetics (19);
N and P are reprinted with permission from
Human Molecular Genetics (20); Q is reprinted with permission from Nature
Genetics (21); and
R is reprinted with permission from Human Molecular
Genetics (24).
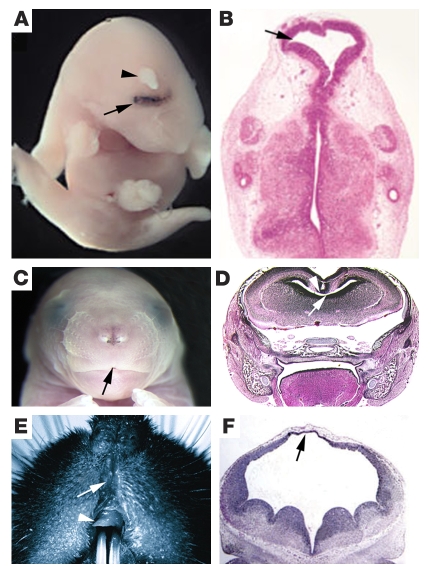
(A and B)
Chd–/–Nog–/–
embryo exhibiting alobar HPE–like phenotype: cyclopia (arrow in
A) and proboscis (arrowhead in A). (B)
Coronal section of
Chd–/–Nog–/–
embryo highlighting the single cerebral ventricle (arrow). (C and
D)
Six3+/kiShh+/– embryos exhibit
semilobar HPE–like phenotype: agenesis of philtrum (arrow in
C), lack of corpus callosum (arrowhead in D), and a
single telencephalic ventricle anteriorly (arrow in D).
(D) Coronal section of a
Six3+/kiShh+/– embryo.
(E) Image of an adult
Cdo–/– mouse exhibiting
microforms of HPE: dysgenesis of philtrum (arrow) and single central maxillary
incisor (arrowhead). (F) Coronal section of an
ShhN/+ embryo exhibiting MIH-like phenotype: lack of dorsal
telencephalic midline structures (arrow in F) and relatively normal
ventral telencephalic structures. A and B are reprinted
with permission from Nature (60); C and D are reprinted with permission from
Developmental Cell (65); E is reprinted with permission from Current
Biology (91); F is
reprinted with permission from Human Molecular Genetics (101).
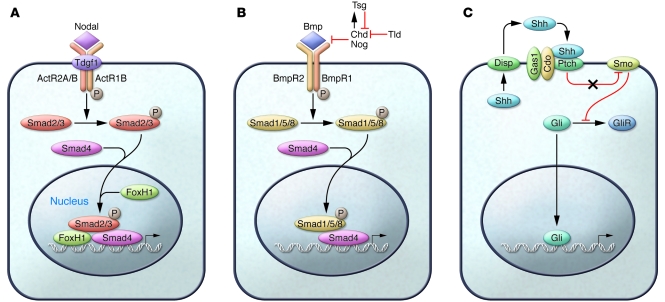
(A) Nodal signaling pathway. (B) Bmp signaling pathway.
(C) Shh signaling pathway. ActR2A, activin A receptor, type 2A;
BmpR2, Bmp receptor 2; Disp, dispatched; Ptch, patched; Smo, smoothened; Tld,
tolloid.
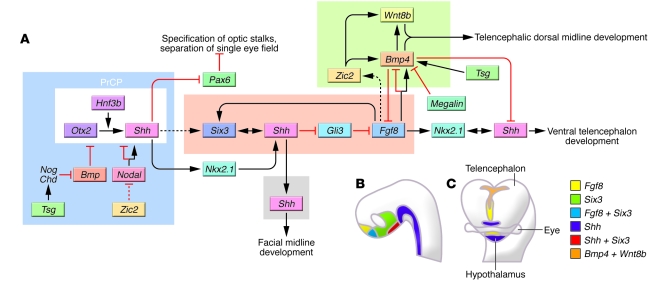
(A) Model of normal mammalian telencephalic development. On the left
side, the PrCP is represented by a white rectangle. The blue square around it
highlights those steps known to be critical in the pathogenesis of alobar HPE.
Toward the right side of the diagram, genes known to be important during
subsequent steps of forebrain development are indicated. The orange rectangle
highlights steps and genes important for semilobar HPE, the green rectangle
highlights those important for MIH, and the gray rectangle highlights those
important for microforms of HPE. Solid lines represent those processes that have
been demonstrated and dashed lines represent those processes that have not yet
been directly proved. To better understand the regional relationships between some
of those critical genes, their normal expression patterns in the telencephalon at
E9.0 and E10.5 are illustrated in B and C, respectively.
C is adapted with permission from Journal of
Neuropathology and Experimental Neurology (106). Hnf3b, hepatocyte nuclear factor
3β; Otx2, orthodenticle homolog 2;
Pax6, paired box gene 6; Wnt8b, wingless-related
MMTV integration site 8b.
References
-
- Robb L., Tam P.P. Gastrula organiser and embryonic patterning in the mouse. Semin. Cell Dev. Biol. 2004;15:543–554. - PubMed
-
- Tam P.P., Loebel D.A. Gene function in mouse embryogenesis: get set for gastrulation. Nat. Rev. Genet. 2007;8:368–381. - PubMed
-
- Rallu M., Corbin J.G., Fishell G. Parsing the prosencephalon. Nat. Rev. Neurosci. 2002;3:943–951. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
