

Prevention of depression in at-risk adolescents: a randomized controlled trial
- PMID: 19491183
- PMCID: PMC2737625
- DOI: 10.1001/jama.2009.788
Prevention of depression in at-risk adolescents: a randomized controlled trial
Abstract
Context: Adolescent offspring of depressed parents are at markedly increased risk of developing depressive disorders. Although some smaller targeted prevention trials have found that depression risk can be reduced, these results have yet to be replicated and extended to large-scale, at-risk populations in different settings.
Objective: To determine the effects of a group cognitive behavioral (CB) prevention program compared with usual care in preventing the onset of depression.
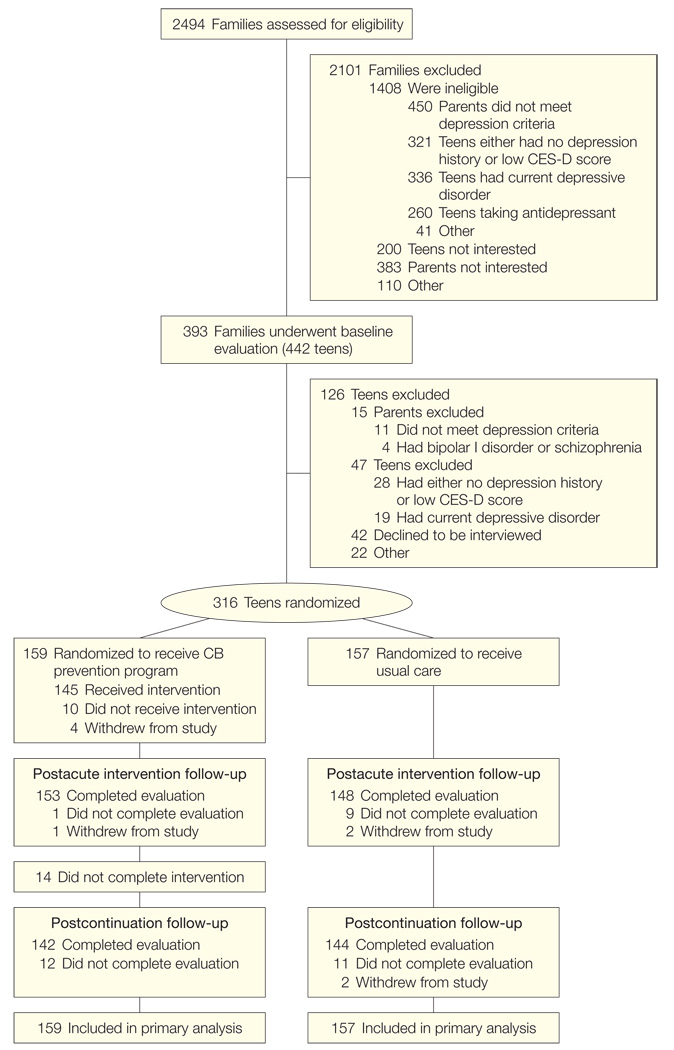
Design, setting, and participants: A multicenter randomized controlled trial conducted in 4 US cities in which 316 adolescent (aged 13-17 years) offspring of parents with current or prior depressive disorders were recruited from August 2003 through February 2006. Adolescents had a past history of depression, current elevated but subdiagnostic depressive symptoms, or both. Assessments were conducted at baseline, after the 8-week intervention, and after the 6-month continuation phase.
Intervention: Adolescents were randomly assigned to the CB prevention program consisting of 8 weekly, 90-minute group sessions followed by 6 monthly continuation sessions or assigned to receive usual care alone.
Main outcome measure: Rate and hazard ratio (HR) of a probable or definite depressive episode (ie, depressive symptom rating score of > or = 4) for at least 2 weeks as diagnosed by clinical interviewers.
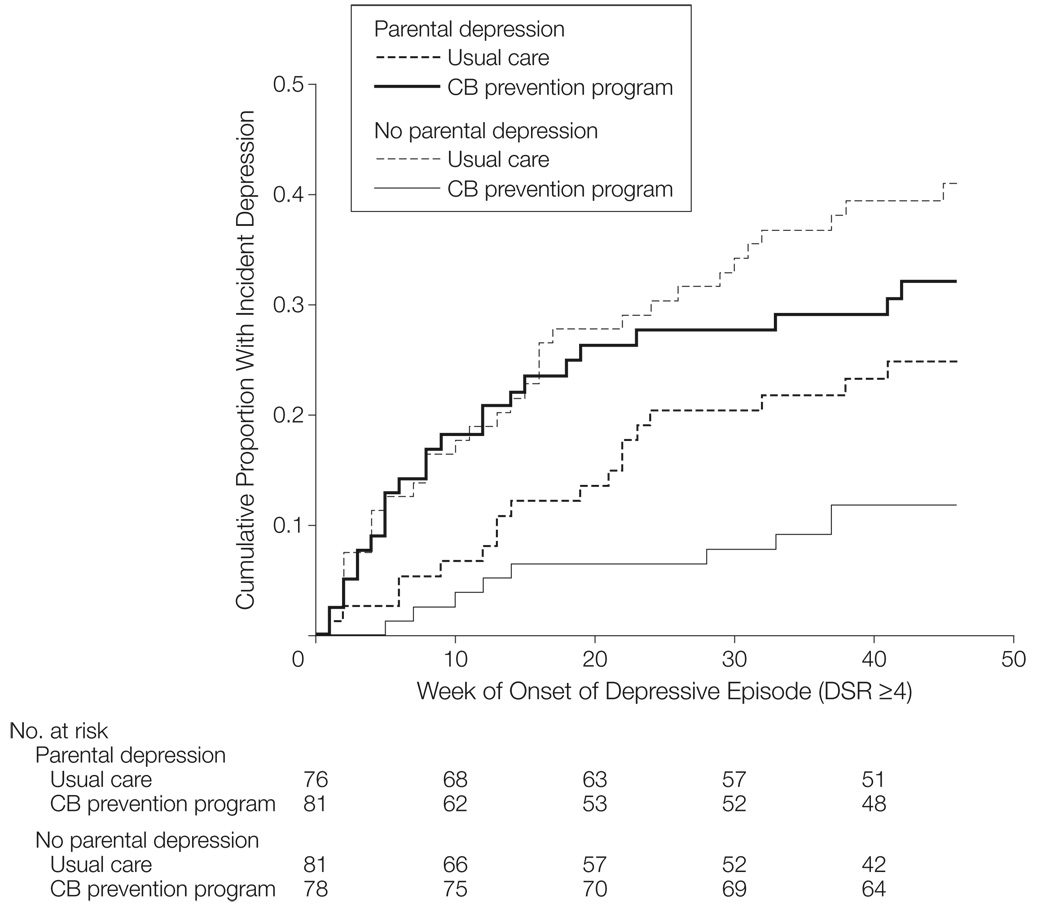
Results: Through the postcontinuation session follow-up, the rate and HR of incident depressive episodes were lower for those in the CB prevention program than for those in usual care (21.4% vs 32.7%; HR, 0.63; 95% confidence interval [CI], 0.40-0.98). Adolescents in the CB prevention program also showed significantly greater improvement in self-reported depressive symptoms than those in usual care (coefficient, -1.1; z = -2.2; P = .03). Current parental depression at baseline moderated intervention effects (HR, 5.98; 95% CI, 2.29-15.58; P = .001). Among adolescents whose parents were not depressed at baseline, the CB prevention program was more effective in preventing onset of depression than usual care (11.7% vs 40.5%; HR, 0.24; 95% CI, 0.11-0.50), whereas for adolescents with a currently depressed parent, the CB prevention program was not more effective than usual care in preventing incident depression (31.2% vs 24.3%; HR, 1.43; 95% CI, 0.76-2.67).
Conclusion: The CB prevention program had a significant prevention effect through the 9-month follow-up period based on both clinical diagnoses and self-reported depressive symptoms, but this effect was not evident for adolescents with a currently depressed parent.
Trial registration: clinicaltrials.gov Identifier: NCT00073671.
Figures

Comment in
-
Health promotion and disease prevention in children: it's never too early.JAMA. 2009 Jun 3;301(21):2270-1. doi: 10.1001/jama.2009.804. JAMA. 2009. PMID: 19491191 No abstract available.
-
Depression in at-risk adolescents and their parents.JAMA. 2009 Sep 16;302(11):1167; author reply 1167-8. doi: 10.1001/jama.2009.1329. JAMA. 2009. PMID: 19755692 Free PMC article. No abstract available.
-
Cognitive behavioral therapy prevents depression in at-risk adolescents.J Pediatr. 2009 Nov;155(5):758. doi: 10.1016/j.jpeds.2009.08.025. J Pediatr. 2009. PMID: 19840623 No abstract available.
-
Group CBT prevents depression in at-risk adolescents.Evid Based Ment Health. 2010 Feb;13(1):16. doi: 10.1136/ebmh.13.1.16. Evid Based Ment Health. 2010. PMID: 20164513 No abstract available.
-
Ignoring the social elements: research of prevention-focused group programs for preadolescents and adolescents.Int J Group Psychother. 2012 Jan;62(1):149-56. doi: 10.1521/ijgp.2012.62.1.149. Int J Group Psychother. 2012. PMID: 22229375 No abstract available.
References
-
- Brent DA, Weersing VR. Depressive disorders in childhood and adolescence. In: Rutter M, Bishop D, Pine D, et al., editors. Rutter’s Child and Adolescent Psychiatry. Oxford, England: Blackwell Publishing Ltd; 2008. pp. 587–613.
-
- Lewinsohn PM, Rohde P, Klein DN, Seeley JR. Natural course of adolescent major depressive disorder, I: continuity into young adulthood. J Am Acad Child Adolesc Psychiatry. 1999;38(1):56–63. - PubMed
-
- Rao U, Hammen C, Daley SE. Continuity of depression during the transition to adulthood: A 5-year longitudinal study of young women. J Am Acad Child Adolesc Psychiatry. 1999;38(7):908–915. - PubMed
-
- Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ. Global and regional burden of disease and risk factors, 2001: systematic analysis of population health data. Lancet. 2006;367(9524):1747–1757. - PubMed
-
- Kennard B, Silva S, Vitiello B, et al. TADS Team. Remission and residual symptoms after short-term treatment in the Treatment of Adolescents with Depression Study (TADS) J Am Acad Child Adolesc Psychiatry. 2006;45(12):1404–1411. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
