

Risk factors for virological failure and subtherapeutic antiretroviral drug concentrations in HIV-positive adults treated in rural northwestern Uganda
- PMID: 19493344
- PMCID: PMC2701435
- DOI: 10.1186/1471-2334-9-81
Risk factors for virological failure and subtherapeutic antiretroviral drug concentrations in HIV-positive adults treated in rural northwestern Uganda
Abstract
Background: Little is known about immunovirological treatment outcomes and adherence in HIV/AIDS patients on antiretroviral therapy (ART) treated using a simplified management approach in rural areas of developing countries, or about the main factors influencing those outcomes in clinical practice.
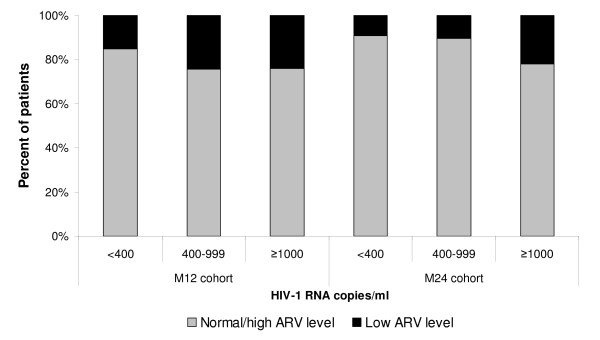
Methods: Cross-sectional immunovirological, pharmacological, and adherence outcomes were evaluated in all patients alive and on fixed-dose ART combinations for 24 months, and in a random sample of those treated for 12 months. Risk factors for virological failure (>1,000 copies/ml) and subtherapeutic antiretroviral (ARV) concentrations were investigated with multiple logistic regression.
Results: At 12 and 24 months of ART, 72% (n = 701) and 70% (n = 369) of patients, respectively, were alive and in care. About 8% and 38% of patients, respectively, were diagnosed with immunological failure; and 75% and 72% of patients, respectively, had undetectable HIV RNA (<400 copies/ml). Risk factors for virological failure (>1,000 copies/ml) were poor adherence, tuberculosis diagnosed after ART initiation, subtherapeutic NNRTI concentrations, general clinical symptoms, and lower weight than at baseline. About 14% of patients had low ARV plasma concentrations. Digestive symptoms and poor adherence to ART were risk factors for low ARV plasma concentrations.
Conclusion: Efforts to improve both access to care and patient management to achieve better immunological and virological outcomes on ART are necessary to maximize the duration of first-line therapy.
Figures

References
-
- UNAIDS. Epidemiological fact sheets on HIV/AIDS and STIs. Uganda; 2008 update. http://www.unaids.org/en/Regions_Countries/Countries/Uganda.asp
-
- DART Virology Group and Trial Team. Virological response to a triple nucleoside/nucleotide analogue regimen over 48 weeks in HIV-1-infected adults in Africa. AIDS. 2006;20:1391–1399. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
