

A comparison of fluoroquinolones versus other antibiotics for treating enteric fever: meta-analysis
- PMID: 19493939
- PMCID: PMC2690620
- DOI: 10.1136/bmj.b1865
A comparison of fluoroquinolones versus other antibiotics for treating enteric fever: meta-analysis
Abstract
Objectives: To review evidence supporting use of fluoroquinolones as first line agents over other antibiotics for treating typhoid and paratyphoid fever (enteric fever).
Design: Meta-analysis of randomised controlled trials.
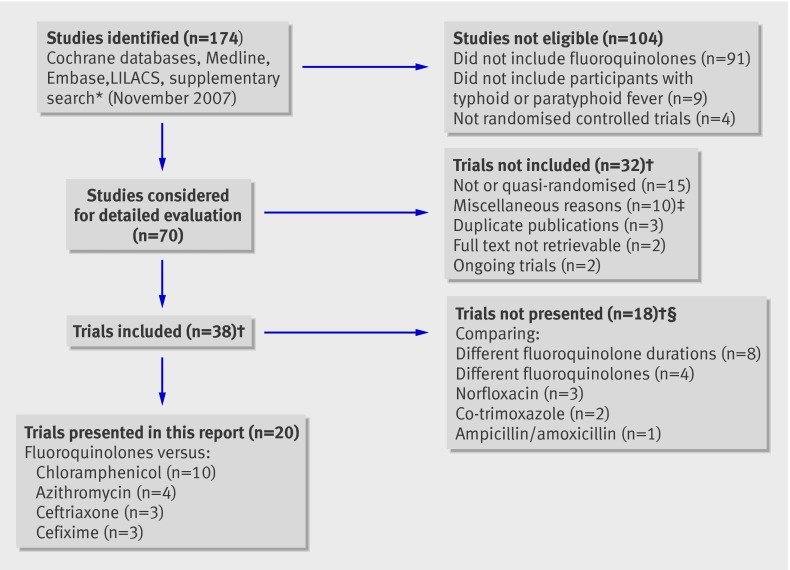
Data sources: Cochrane Infectious Diseases Group specialised register, CENTRAL (issue 4, 2007), Medline (1966-2007), Embase (1974-2007), LILACS (1982-2007), selected conferences, reference lists, and ongoing trial register (November 2007). Review methods Trials comparing fluoroquinolones with chloramphenicol, cephalosporins, or azithromycin in culture-proven enteric fever were included. Two reviewers extracted data and assessed methodological quality. Odds ratios with 95% confidence intervals were estimated. Trials recruiting over 60% children were analysed separately from trials on adults. Primary outcomes studied were clinical failure, microbiological failure, and relapse.
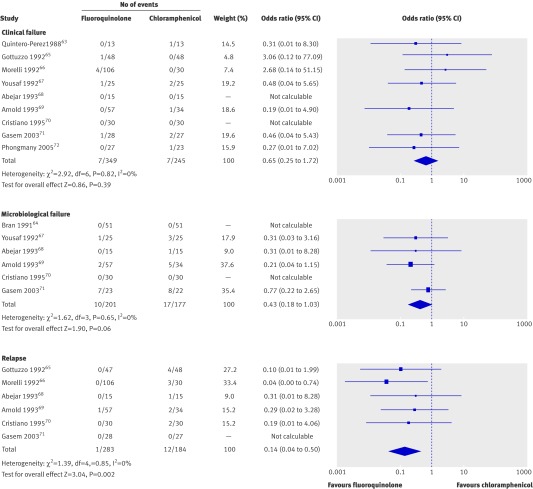
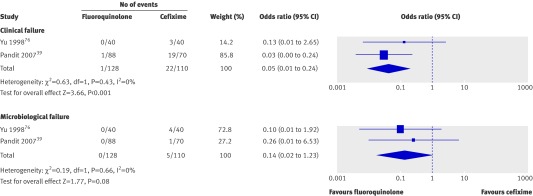
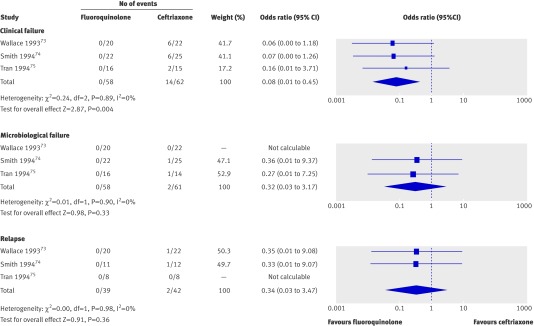
Results: Twenty trials were included. Trials were small and often of limited methodological quality. Only 10 trials concealed allocation and only three were blinded. In trials on adults, fluoroquinolones were not significantly different from chloramphenicol for clinical failure (594 participants) or microbiological failure (n=378), but reduced clinical relapse (odds ratio 0.14 (95% confidence interval 0.04 to 0.50), n=467, 6 trials). Azithromycin and fluoroquinolones were comparable (n=152, 2 trials). Compared with ceftriaxone, fluoroquinolones reduced clinical failure (0.08 (0.01 to 0.45), n=120, 3 trials) but not microbiological failure or relapse. Compared with cefixime, fluoroquinolones reduced clinical failure (0.05 (0.01 to 0.24), n=238, 2 trials) and relapse (0.18 (0.03 to 0.91), n=218, 2 trials). In trials on children infected with nalidixic acid resistant strains, older fluoroquinolones (ofloxacin) produced more clinical failures than azithromycin (2.67 (1.16 to 6.11), n=125, 1 trial), but there were no differences with newer fluoroquinolones (gatifloxacin, n=285, 1 trial). Fluoroquinolones and cefixime were not significantly different (n=82, 1 trial).
Conclusions: In adults, fluoroquinolones may be better than chloramphenicol for preventing clinical relapse. Data were limited for other comparisons, particularly for children.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Treatment of enteric fever.BMJ. 2009 Jun 3;338:b1159. doi: 10.1136/bmj.b1159. BMJ. 2009. PMID: 19493937 No abstract available.
References
-
- Sinha A, Sazawal S, Kumar R, Sood S, Reddaiah VP, Singh B, et al. Typhoid fever in children aged less than 5 years. Lancet 1999;354:734-7. - PubMed
-
- Lin FY, Vo AH, Phan VB, Nguyen TT, Bryla D, Tran CT, et al. The epidemiology of typhoid fever in the Dong Thap Province, Mekong Delta region of Vietnam. Am J Trop Med Hyg 2000;62:644-8. - PubMed
-
- Saha SK, Baqui AH, Hanif M, Darmstadt GL, Ruhulamin M, Nagatake T, et al. Typhoid fever in Bangladesh: implications for vaccination policy. Pediatr Infect Dis J 2001;20:521-4. - PubMed
-
- Saha MR, Dutta P, Palit A, Dutta D, Bhattacharya MK, Mitra U, et al. A note on incidence of typhoid fever in diverse age groups in Kolkata, India. Jpn J Infect Dis 2003;56:121-2. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical