

An autoinflammatory disease due to homozygous deletion of the IL1RN locus
- PMID: 19494219
- PMCID: PMC2803085
- DOI: 10.1056/NEJMoa0809568
An autoinflammatory disease due to homozygous deletion of the IL1RN locus
Abstract
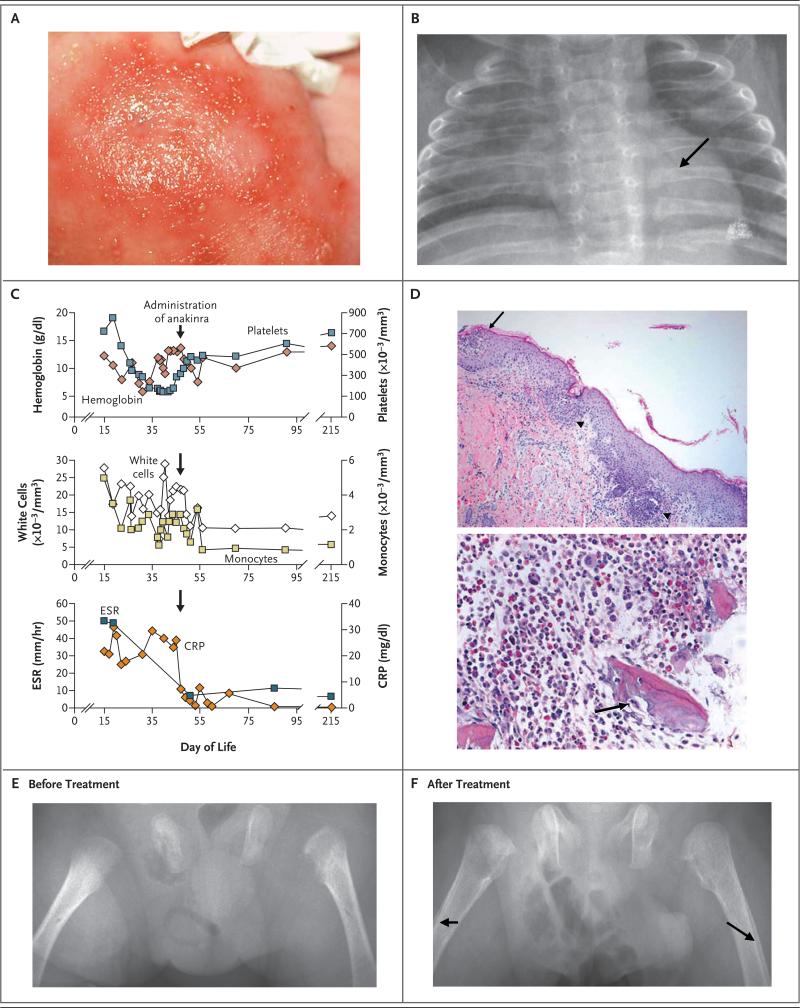
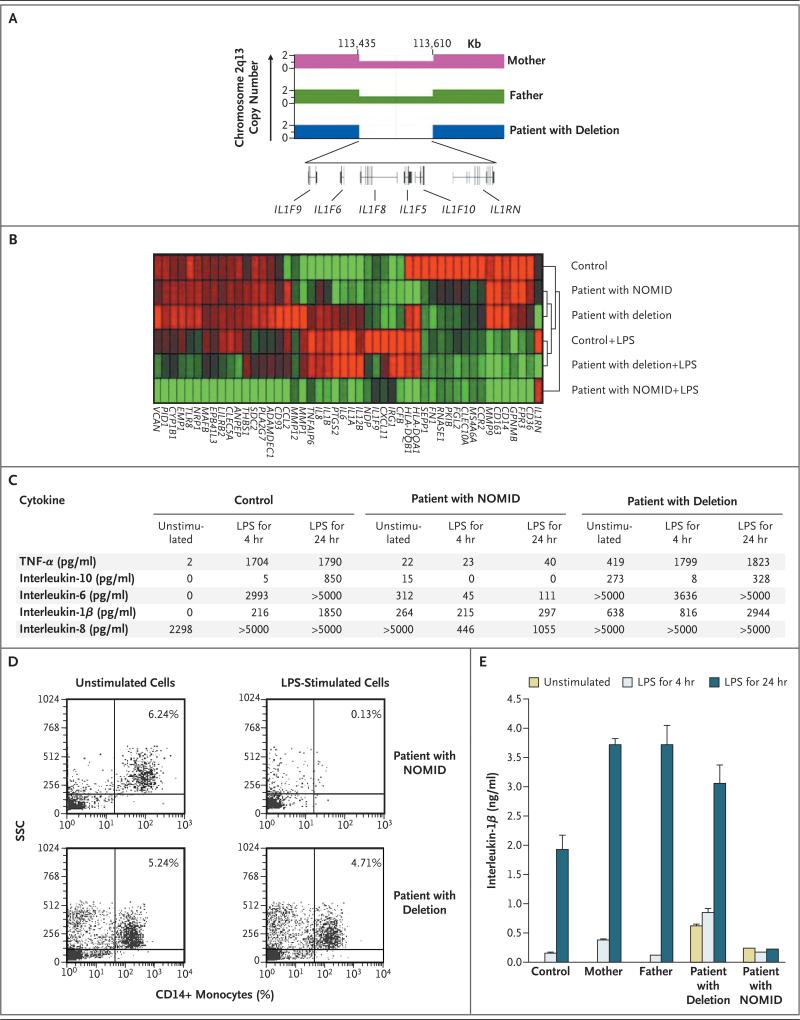
We describe a patient with an autoinflammatory disease in which the main clinical features are pustular rash, marked osteopenia, lytic bone lesions, respiratory insufficiency, and thrombosis. Genetic studies revealed a 175-kb homozygous deletion at chromosome 2q13, which encompasses several interleukin-1 family members, including the gene encoding the interleukin-1-receptor antagonist (IL1RN). Mononuclear cells, obtained from the patient and cultured, produced large amounts of inflammatory cytokines, with increasing amounts secreted after stimulation with lipopolysaccharide. A similar increase was not observed in peripheral-blood mononuclear cells from a patient with neonatal-onset multisystem inflammatory disorder (NOMID). Treatment with anakinra completely resolved the symptoms and lesions.
2009 Massachusetts Medical Society
Figures
Comment in
-
Interleukin-1beta and the autoinflammatory diseases.N Engl J Med. 2009 Jun 4;360(23):2467-70. doi: 10.1056/NEJMe0811014. N Engl J Med. 2009. PMID: 19494224 No abstract available.
References
-
- Hull KM, Shoham N, Chae JJ, Aksentijevich I, Kastner DL. The expanding spectrum of systemic autoinflammatory disorders and their rheumatic manifestations. Curr Opin Rheumatol. 2003;15:61–9. - PubMed
-
- Prieur AM, Griscelli C. Arthropathy with rash, chronic meningitis, eye lesions, and mental retardation. J Pediatr. 1981;99:79–83. - PubMed
-
- Prieur AM, Griscelli C, Lampert F, et al. A chronic, infantile, neurological, cutaneous and articular (CINCA) syndrome: a specific entity analysed in 30 patients. Scand J Rheumatol Suppl. 1987;66:57–68. - PubMed
-
- Aksentijevich I, Nowak M, Mallah M, et al. De novo CIAS1 mutations, cytokine activation, and evidence for genetic heterogeneity in patients with neonatal-onset multi-system inflammatory disease (NOMID): a new member of the expanding family of pyrin-associated autoinflammatory diseases. Arthritis Rheum. 2002;46:3340–8. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical