

ACE (I/D) polymorphism and response to treatment in coronary artery disease: a comprehensive database and meta-analysis involving study quality evaluation
- PMID: 19497121
- PMCID: PMC2700093
- DOI: 10.1186/1471-2350-10-50
ACE (I/D) polymorphism and response to treatment in coronary artery disease: a comprehensive database and meta-analysis involving study quality evaluation
Abstract
Background: The role of angiotensin-converting enzyme (ACE) gene insertion/deletion (I/D) polymorphism in modifying the response to treatment modalities in coronary artery disease is controversial.
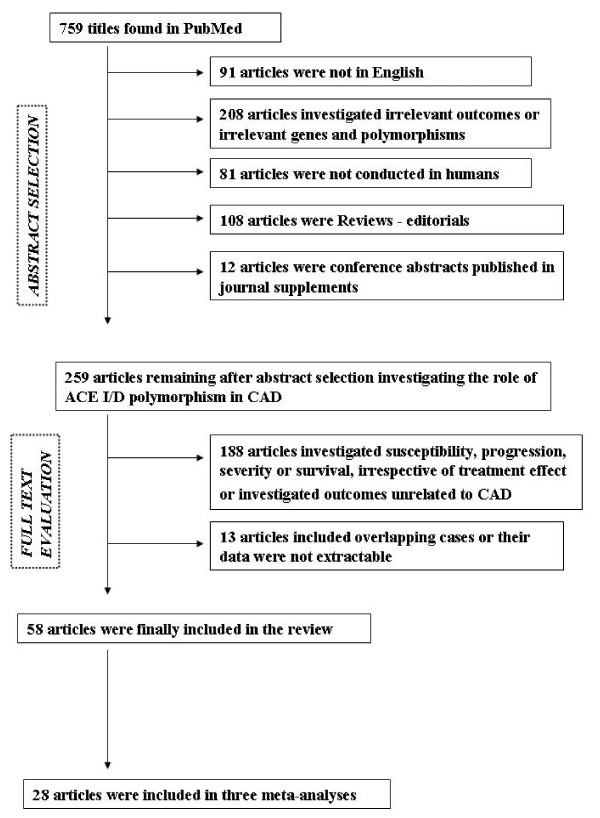
Methods: PubMed was searched and a database of 58 studies with detailed information regarding ACE I/D polymorphism and response to treatment in coronary artery disease was created. Eligible studies were synthesized using meta-analysis methods, including cumulative meta-analysis. Heterogeneity and study quality issues were explored.
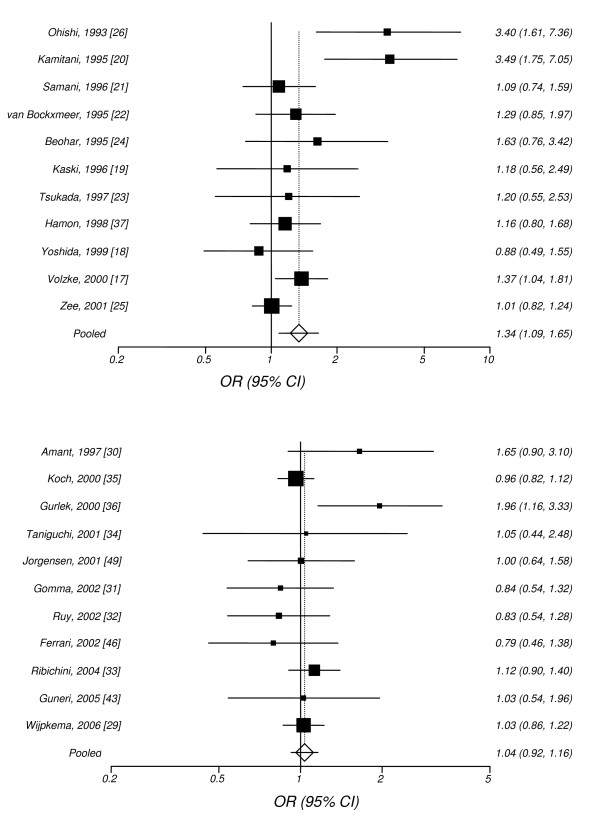
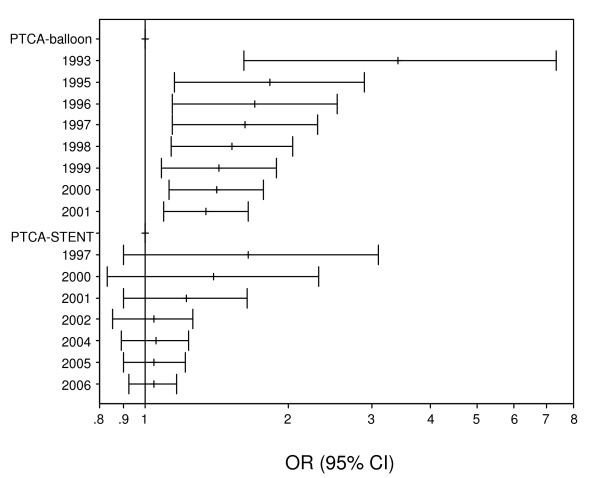
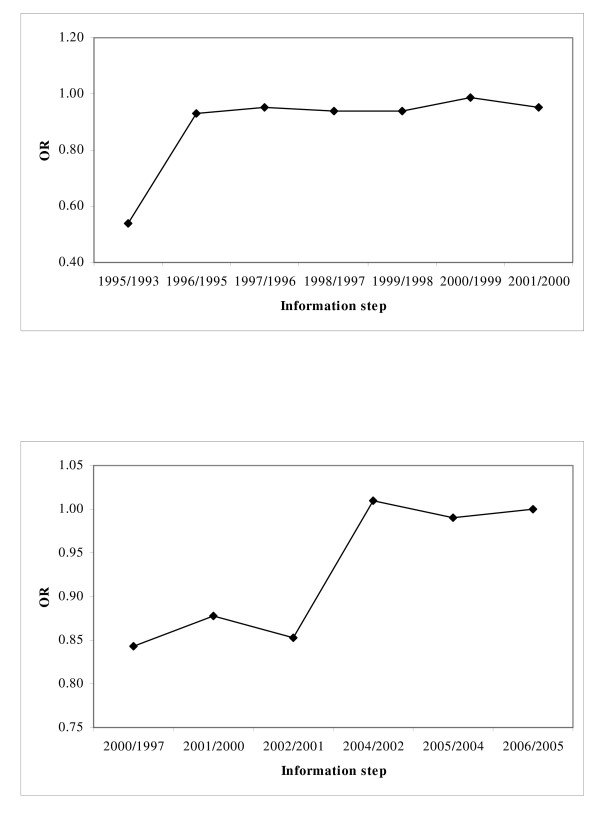
Results: Forty studies involved invasive treatments (coronary angioplasty or coronary artery by-pass grafting) and 18 used conservative treatment options (including anti-hypertensive drugs, lipid lowering therapy and cardiac rehabilitation procedures). Clinical outcomes were investigated by 11 studies, while 47 studies focused on surrogate endpoints. The most studied outcome was the restenosis following coronary angioplasty (34 studies). Heterogeneity among studies (p < 0.01) was revealed and the risk of restenosis following balloon angioplasty was significant under an additive model: the random effects odds ratio was 1.42 (95% confidence interval:1.07-1.91). Cumulative meta-analysis showed a trend of association as information accumulates. The results were affected by population origin and study quality criteria. The meta-analyses for the risk of restenosis following stent angioplasty or after angioplasty and treatment with angiotensin-converting enzyme inhibitors produced non-significant results. The allele contrast random effects odds ratios with the 95% confidence intervals were 1.04(0.92-1.16) and 1.10(0.81-1.48), respectively. Regarding the effect of ACE I/D polymorphism on the response to treatment for the rest outcomes (coronary events, endothelial dysfunction, left ventricular remodeling, progression/regression of atherosclerosis), individual studies showed significance; however, results were discrepant and inconsistent.
Conclusion: In view of available evidence, genetic testing of ACE I/D polymorphism prior to clinical decision making is not currently justified. The relation between ACE genetic variation and response to treatment in CAD remains an unresolved issue. The results of long-term and properly designed prospective studies hold the promise for pharmacogenetically tailored therapy in CAD.
Figures
References
-
- Arnett DK, Baird AE, Barkley RA, Basson CT, Boerwinkle E, Ganesh SK, Herrington DM, Hong Y, Jaquish C, McDermott DA, O'Donnell CJ, American Heart Association Council on Epidemiology and Prevention; American Heart Association Stroke Council; Functional Genomics and Translational Biology Interdisciplinary Working Group Relevance of genetics and genomics for prevention and treatment of cardiovascular disease: a scientific statement from the American Heart Association Council on Epidemiology and Prevention, the Stroke Council, and the Functional Genomics and Translational Biology Interdisciplinary Working Group. Circulation. 2007;115:2878–2901. doi: 10.1161/CIRCULATIONAHA.107.183679. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
