

Number needed to treat to benefit and to harm for intravenous tissue plasminogen activator therapy in the 3- to 4.5-hour window: joint outcome table analysis of the ECASS 3 trial
- PMID: 19498197
- PMCID: PMC2724988
- DOI: 10.1161/STROKEAHA.108.543561
Number needed to treat to benefit and to harm for intravenous tissue plasminogen activator therapy in the 3- to 4.5-hour window: joint outcome table analysis of the ECASS 3 trial
Abstract
Background and purpose: Measures of a therapy's effect size are important guides to clinicians, patients, and policy-makers on treatment decisions in clinical practice. The ECASS 3 trial demonstrated a statistically significant benefit of intravenous tissue plasminogen activator for acute cerebral ischemia in the 3- to 4.5-hour window, but an effect size estimate incorporating benefit and harm across all levels of poststroke disability has not previously been derived.
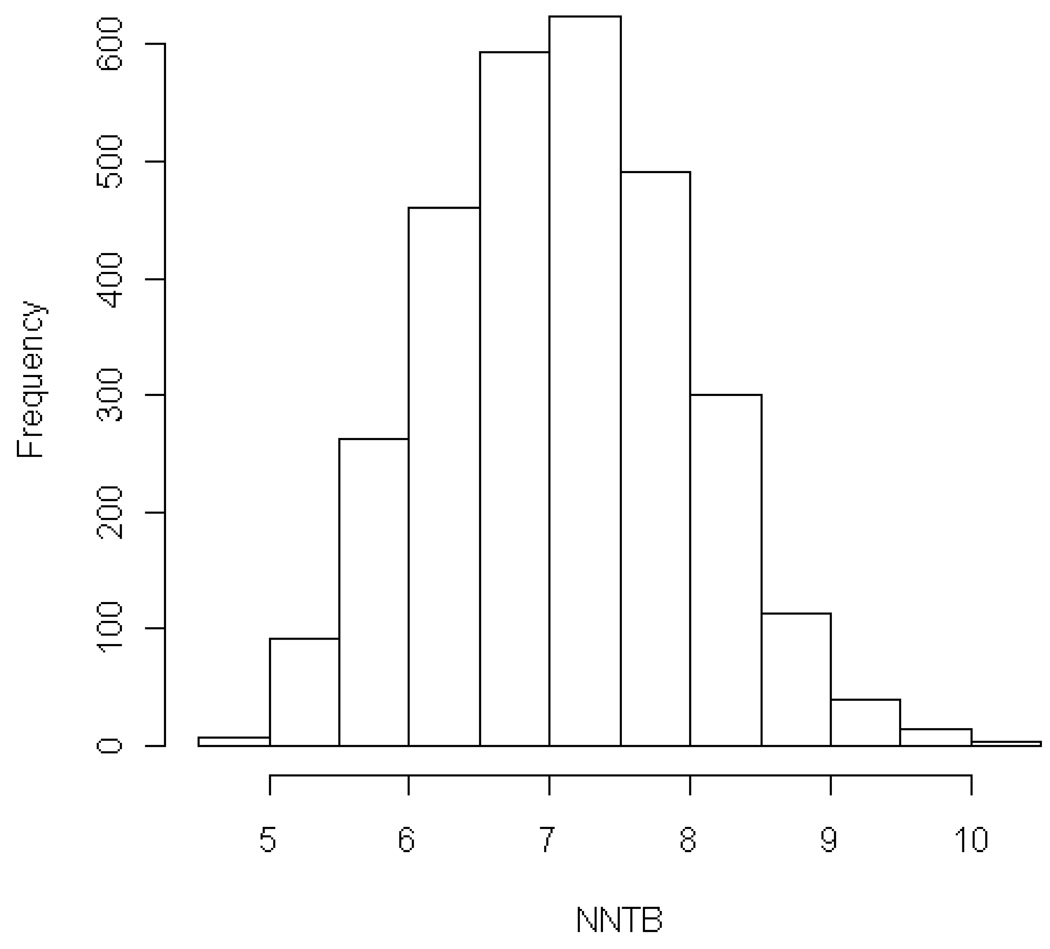
Methods: Joint outcome table specification was used to derive number needed to treat to benefit (NNTB) and number needed to treat to harm (NNTH) values summarizing treatment impact over the entire outcome range on the modified Rankin scale of global disability, including both expert-dependent and expert-independent (algorithmic and repeated random sampling) array generation.
Results: For the full 7-category modified Rankin scale, algorithmic analysis demonstrated that the NNTB for 1 additional patient to have a better outcome by >or=1 grades than with placebo must lie between 4.0 and 13.0. In bootstrap simulations, the mean NNTB was 7.1. Expert joint outcome table analyses indicated that the NNTB for improved final outcome was 6.1 (95% CI, 5.6-6.7) and the NNTH 37.5 (95% CI, 34.6-40.5). Benefit per 100 patients treated was 16.3 and harm per 100 was 2.7. The likelihood of help to harm ratio was 6.0.
Conclusions: Treatment with tissue plasminogen activator in the 3- to 4.5-hour window confers benefit on approximately half as many patients as treatment <3 hours, with no increase in the conferral of harm. Approximately 1 in 6 patients has a better and 1 in 35 has a worse outcome as a result of therapy.
Figures
Comment in
-
Treating patients with ischemic stroke with tissue plasminogen activator in the 3.5- to 4-hour window: numbers support benefit but the message is to still go fast.Stroke. 2009 Jul;40(7):2295-6. doi: 10.1161/STROKEAHA.109.552398. Epub 2009 Jun 4. Stroke. 2009. PMID: 19498185 No abstract available.
References
-
- Saver JL. Time is brain--quantified. Stroke. 2006;37:263–266. - PubMed
-
- Marler JR, Tilley BC, Lu M, et al. Early stroke treatment associated with better outcome: the NINDS rt-PA stroke study. Neurology. 2000;55:1649–1655. - PubMed
-
- Wardlaw J, del Zoppo G, Yamaguchi T, Berge E. Thrombolysis for acute ischaemic stroke. Cochrane Database of Systematic Reviews. 2003 - PubMed
-
- Saver JL, Kidwell CS, Starkman S. Commentary: Thrombolysis in stroke: it works! British Medical Journal. 2002;324:727–729.
-
- Hacke W, Donnan G, Fieschi C, et al. Association of outcome with early stroke treatment: pooled analysis of ATLANTIS, ECASS, and NINDS rt-PA stroke trials. Lancet. 2004;363:768–774. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
