

Patent foramen ovale, cardiac valve thickening, and antiphospholipid antibodies as risk factors for subsequent vascular events: the PICSS-APASS study
- PMID: 19498198
- PMCID: PMC2761081
- DOI: 10.1161/STROKEAHA.108.539171
Patent foramen ovale, cardiac valve thickening, and antiphospholipid antibodies as risk factors for subsequent vascular events: the PICSS-APASS study
Abstract
Background and purpose: We sought to estimate risk of recurrent stroke/TIA/death in the subgroup of the Patent Foramen Ovale in the Cryptogenic Stroke Study (PICSS) cohort with patent foramen ovale (PFO) and antiphospholipid antibodies (aPL) and to estimate risk of recurrent stroke/TIA/death in aPL-positive patients who have thickened left-side heart valves (VaT). PFO is associated with cryptogenic ischemic stroke. Also, the presence of aPL is associated with ischemic cerebrovascular disease.
Methods: Combined data from 2 major substudies of the Warfarin Aspirin Recurrent Stroke Trial (WARSS) were evaluated. PICSS subjects were included if they were enrolled in the Antiphospholipid Antibodies and Stroke Study (APASS) and underwent a baseline aPL test (lupus anticoagulant, anticardiolipin antibodies, or both) within 1 month of the stroke. All patients in PICSS underwent transesophageal echocardiography for PFO as well as VaT, which was performed blinded to aPL status and treatment arm (325 mg/day aspirin or adjusted dose warfarin; target international normalized ratio, 1.4-2.8). The primary outcome event was the 2-year risk of recurrent stroke/TIA/death and was evaluated using Cox proportional hazards model. Because there was no treatment effect, warfarin and aspirin groups were combined to increase power. For the combined end point, power to detect HR of 2 was 47.8% for the PFO and aPL-positive group, and 75.3% for the valve thickening and aPL-positive group, assuming 2-sided type I error of 0.05.
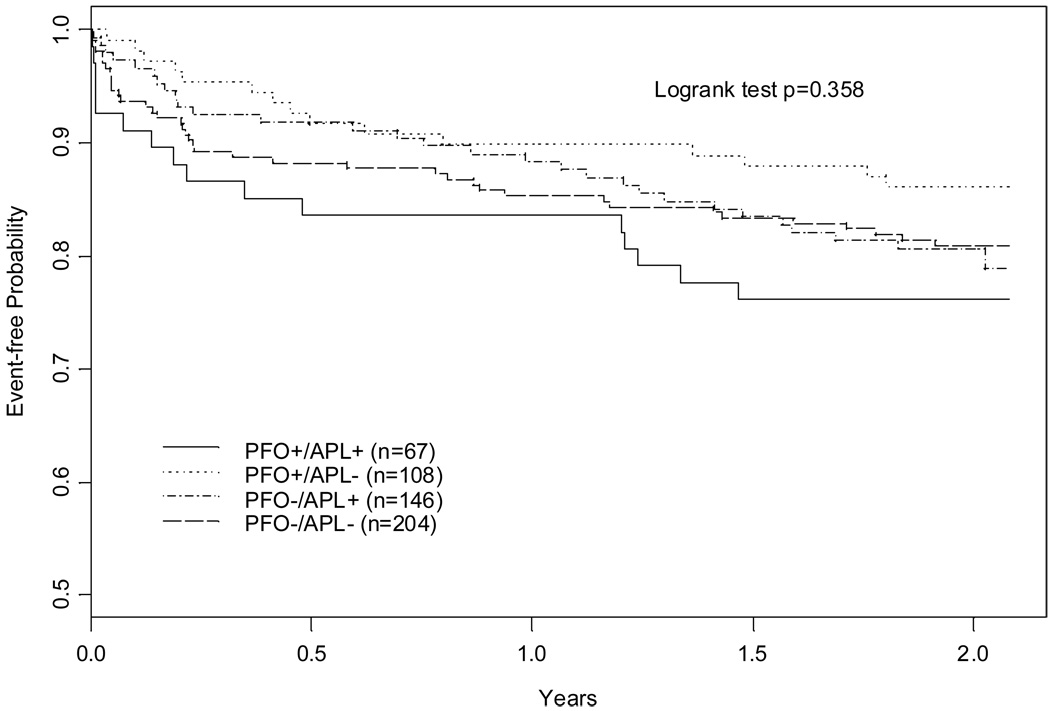
Results: Five hundred twenty-five subjects were tested for the combined presence of PFO and aPL and were available for evaluation. The primary outcome event rate was 23.9% (HR, 1.39; 95% CI, 0.75-2.59) in the PFO-positive/aPL-positive group, compared to 13.9% (HR, 0.83; 95% CI, 0.44-1.56) in the PFO-positive/aPL-negative group, and 19.9% (HR, 1.16; 95% CI, 0.68-1.90) in the PFO-negative/aPL-positive group. Five hundred forty-five subjects tested for combined presence of aPL and left-side cardiac VaT were available for evaluation. The primary event rate was 22.6% (HR, 1.65; 95% CI, 0.88-3.09) in the VaT-positive/aPL-positive group, compared to 19.4% (HR, 1.50; 95% CI, 0.82-2.75) in the VaT-positive/aPL-negative group, and 20.2% (HR, 1.63; 95% CI, 0.81-3.25) in the VaT-negative/aPL-positive group.
Conclusions: The combined presence of aPL either with a PFO or with left-side cardiac VaT did not significantly increase risk of subsequent cerebrovascular events in this PICCS/APASS cohort of patients.
Figures

References
-
- Sacco RL, Ellenberg JH, Mohr JP, Tatemichi TK, Hier DB, Price TR, Wolf PA. Infarcts of undetermined cause: The NINCDS stroke data bank. Annals of Neurology. 1989;25(4):382–390. - PubMed
-
- Lechat P, Mas JL, Lascault G, Loron P, Theard M, Klimczac M, Drobinski G, Thomas D, Grosgogeat Y. Prevalence of patent foramen ovale in patients with stroke. N Engl J Med. 1988;318(18):1148–1152. - PubMed
-
- Cabanes L, Mas JL, Cohen A, Amerenco P, Cabanes PA, Oubary P, Chedru F, Guerin F, Bousser MG, de Recondo J. Atrial septal aneurysm and patent foramen ovale as risk factors for cryptogenic stroke in patients less than 55 years of age. A study using transesophageal echocardiography. Stroke. 1993;24(12):1865–1873. - PubMed
-
- Hausmann D, Mugge A, Daniel WG. Identification of patent foramen ovale permitting paradoxic embolism. J Am Coll Cardiol. 1995;26(4):1030–1038. - PubMed
-
- Webster MWI, Smith HJ, Sharpe DN, Chancellor AM, Swift DL, Bass NM, Glasgow GL. Patent Foramen ovale in young stroke patients. Lancet. 1988;332(8601):11. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
