

Description of clinical risk factor changes during naturopathic care for type 2 diabetes
- PMID: 19500011
- PMCID: PMC3046878
- DOI: 10.1089/acm.2008.0249
Description of clinical risk factor changes during naturopathic care for type 2 diabetes
Abstract
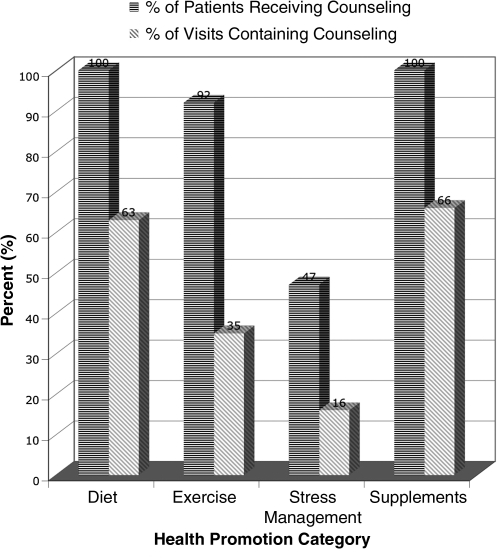
Background: Survey findings report that 48% of people with type 2 diabetes use complementary and alternative medicine (CAM) practice. Publications suggest a high incidence of health promotion counseling in naturopathic practice, yet clinical data on risk factor changes are not available in the literature.
Objectives: The primary aim of this study was to describe clinical risk factor changes during the utilization of naturopathic CAM services in patients with type 2 diabetes.
Design: A retrospective, observational study design was used to describe naturopathic care.
Setting: Abstracted medical charts were from patients of the Bastyr Center for Natural Health in Seattle, WA.
Participants: The patients in this study had type 2 diabetes and received naturopathic care between 2001 and 2006.
Outcomes: Abstracted data included patient demographics, duration of care, number of visits, laboratory values for hemoglobin A1c (HbA1c), low density lipoprotein (LDL) and high density lipoprotein (HDL) cholesterol, triglycerides (TAG); and systolic/diastolic blood pressure (SPB, DBP).
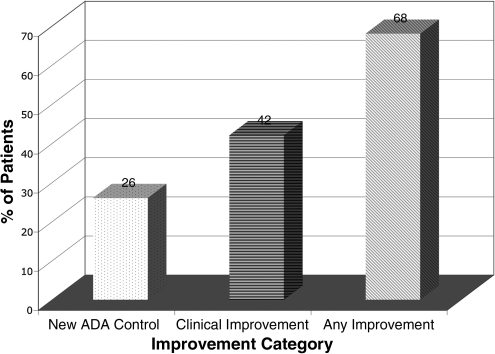
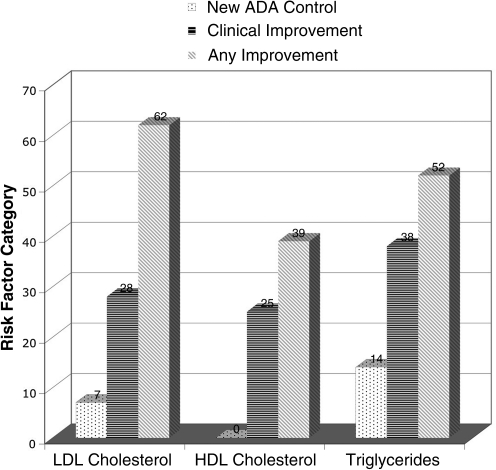
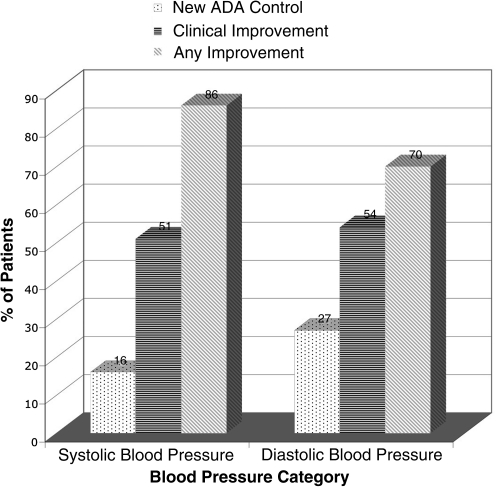
Results: Thirty-seven (37) patient records met inclusion criteria and were abstracted in detail. Mean and median duration of care were 27 and 20 months, respectively. The mean number of visits was 11. Significant mean changes in clinical laboratory risk factors over the duration of care were: -0.65% for HbA1c (p = 0.046), -45 mg/dL for TAG (p = 0.037), -7 mm Hg in SBP (p = 0.02), and -5 mm Hg in DBP (p = 0.003). Mean changes for cholesterol did not reach statistical significance. The percentage of patients who reached new control, had clinically significant risk factor improvements, or had any improvement was: 26%, 42%, and 68% for HbA1c, 7%, 28%, and 62% for LDL, 0%, 25%, and 39% for HDL, 14%, 38%, and 52% for TAG, 16%, 51%, and 86% for SBP, and 27%, 54%, and 70% for DBP. COMMENTS/CONCLUSIONS: These preliminary outcomes suggest that risk factor improvements occur during naturopathic care for diabetes, although the contribution of naturopathic care to these changes cannot be determined. Effectiveness and generalizability of naturopathic approaches in treating type 2 diabetes should be evaluated in controlled prospective studies in representative populations or randomized trials.
Figures
References
-
- American Diabetes Association. Economic costs of diabetes in the U.S. in 2007. Diabetes Care. 2008;31:597. - PubMed
-
- Wee CC, et al. Physician counseling about exercise. JAMA. 1999;282:1583–1588. - PubMed
-
- Heaton PC. Frede SM. Patients' need for more counseling on diet, exercise, and smoking cessation: Results from the National Ambulatory Medical Care Survey (2003) J Am Pharm Assoc. 2006;46:364–369. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
