

Decreased upright cerebral blood flow and cerebral autoregulation in normocapnic postural tachycardia syndrome
- PMID: 19502561
- PMCID: PMC2724195
- DOI: 10.1152/ajpheart.00138.2009
Decreased upright cerebral blood flow and cerebral autoregulation in normocapnic postural tachycardia syndrome
Abstract
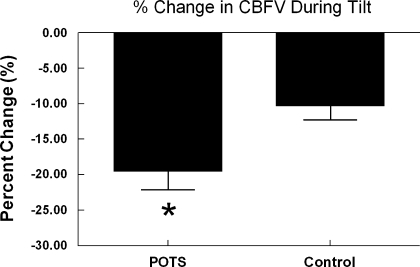
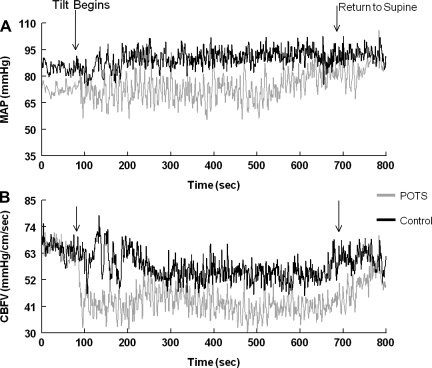
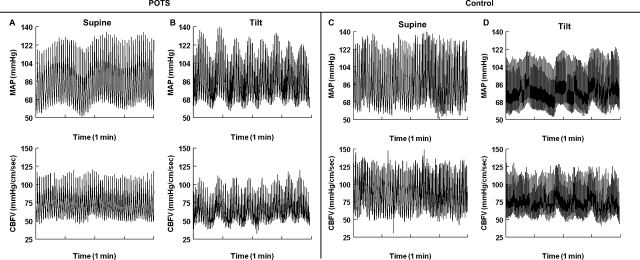
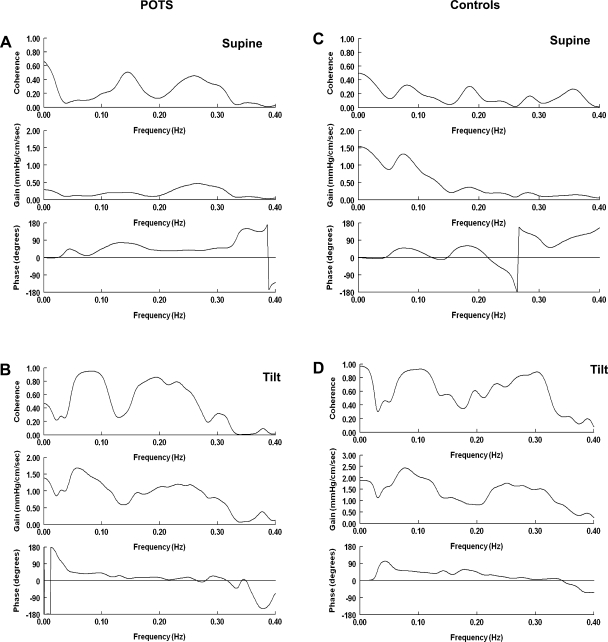
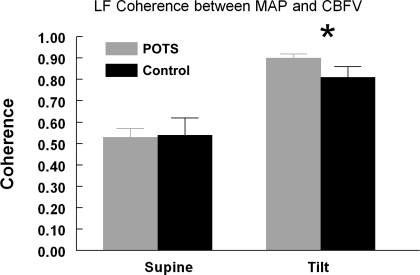
Postural tachycardia syndrome (POTS), a chronic form of orthostatic intolerance, has signs and symptoms of lightheadedness, loss of vision, headache, fatigue, and neurocognitive deficits consistent with reductions in cerebrovascular perfusion. We hypothesized that young, normocapnic POTS patients exhibit abnormal cerebral autoregulation (CA) that results in decreased static and dynamic cerebral blood flow (CBF) autoregulation. All subjects had continuous recordings of mean arterial pressure (MAP) and CBF velocity (CBFV) using transcranial Doppler sonography in both the supine supine position and during a 70 degrees head-up tilt. During tilt, POTS patients (n = 9) demonstrated a higher heart rate than controls (n = 7) (109 +/- 6 vs. 80 +/- 2 beats/min, P < 0.05), whereas controls demonstrated a higher MAP than POTS (87 +/- 2 vs. 77 +/- 3 mmHg, P < 0.05). Also during tilt, mean CBFV decreased 19.5 +/- 2.6% in POTS patients versus 10.3 +/- 2.0% in controls (P < 0.05). We then used a transfer function analysis of MAP and CFBV in the frequency domain to quantify these changes. The low-frequency (LF; 0.04-0.15 Hz) component of CBFV variability increased during tilt in POTS patients (supine: 3 +/- 0.9 vs. tilt: 9 +/- 2, P < 0.02). In POTS patients, there was an increase in LF and high-frequency coherence between MAP and CBFV, an increase in LF gain, and a lack of significant change in phase. Static CA may be less effective in POTS patients compared with controls, since immediately after tilt CBFV decreased more in POTS patients and was highly oscillatory and autoregulation did not restore CBFV to baseline values until the subjects became supine. Dynamic CA may be less effective in POTS patients because MAP and CBFV during tilt became almost perfectly synchronous. We conclude that dynamic and static autoregulation of CBF are less effective in POTS patients compared with control subjects during orthostatic challenge.
Figures
References
-
- Baumbach GL, Heistad DD. Regional, segmental, and temporal heterogeneity of cerebral vascular autoregulation. Ann Biomed Eng 13: 303–310, 1985. - PubMed
-
- Bendat JS, Piersol AG. Random Data Analysis and Measurement Procedures. New York: Wiley-Interscience, 1971.
-
- Bevan RD, Dodge J, Nichols P, Penar PL, Walters CL, Wellman T, Bevan JA. Weakness of sympathetic neural control of human pial compared with superficial temporal arteries reflects low innervation density and poor sympathetic responsiveness. Stroke 29: 212–221, 1998. - PubMed
-
- Birch AA, Dirnhuber MJ, Hartley-Davies R, Iannotti F, Neil-Dwyer G. Assessment of autoregulation by means of periodic changes in blood pressure. Stroke 26: 834–837, 1995. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical