

Antithrombotic therapy and outcomes of patients with atrial fibrillation following primary percutaneous coronary intervention: results from the APEX-AMI trial
- PMID: 19502623
- PMCID: PMC2764954
- DOI: 10.1093/eurheartj/ehp213
Antithrombotic therapy and outcomes of patients with atrial fibrillation following primary percutaneous coronary intervention: results from the APEX-AMI trial
Abstract
Aims: To assess the incidence and timing of atrial fibrillation (AF), describe antithrombotic therapy use, and evaluate the association of AF with 90 day mortality and other secondary clinical outcomes.
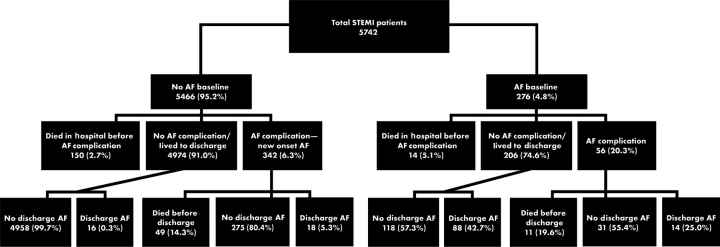
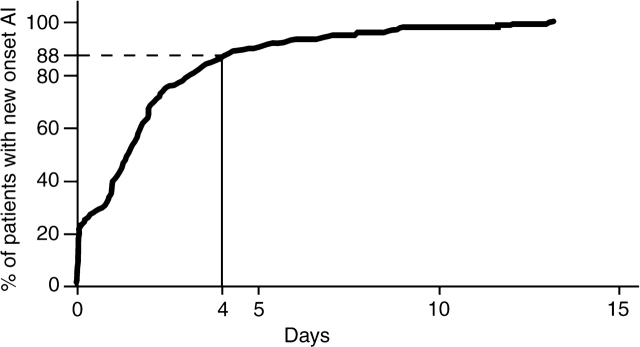
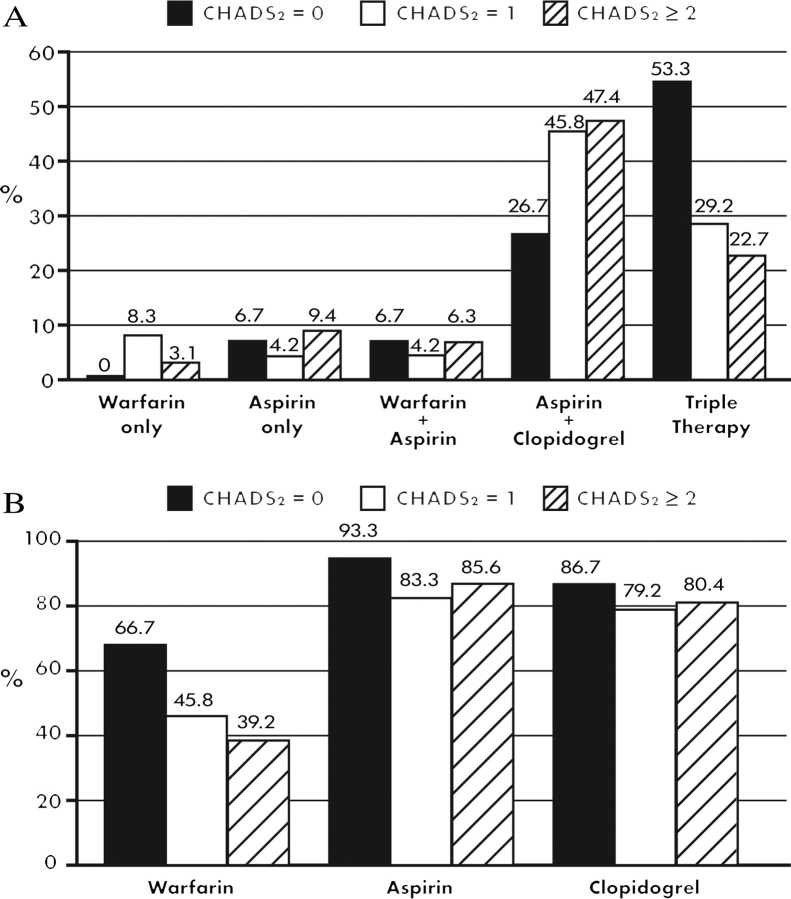
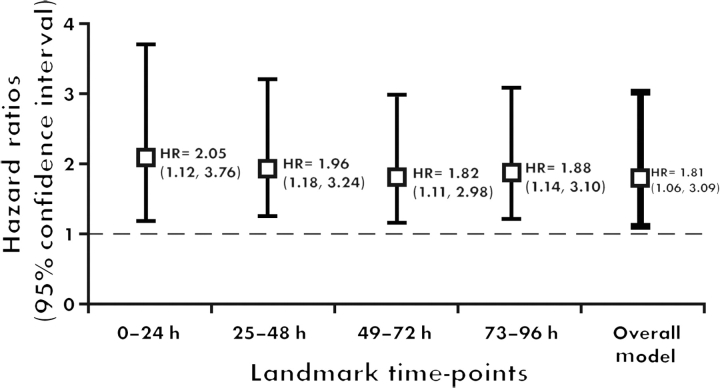
Methods and results: We studied 5745 ST-segment elevation myocardial infarction patients treated with primary percutaneous coronary intervention (PCI) in APEX-AMI. Approximately 11% had AF during hospitalization. Atrial fibrillation prevalence at baseline and at discharge was 4.8% [confidence interval (CI) 4.3-5.4%] and 2.5% (CI 2.1-2.9%), respectively. The proportion of 5466 patients without AF at baseline who developed new onset AF was 6.3% (CI 5.6-6.9%). This corresponded to 9.3 cases of new onset AF/1000 patient days at risk. New onset AF was independently associated with 90 day mortality [adjusted hazard ratio (HR) 1.81; 95% CI 1.06-3.09; P = 0.029] after accounting for baseline covariates and in-hospital procedures and complications. New onset AF was associated with shock (adjusted HR 3.81; 95% CI 1.88-7.70; P = 0.0002), congestive heart failure (adjusted HR 2.66; 95% CI 1.74-4.06; P < 0.0001), and stroke (adjusted HR 2.98; 95% CI 1.47-6.04; P = 0.0024) in models accounting for baseline covariates. Of AF patients, 55% did not receive oral anticoagulation therapy at discharge. Among patients with coronary stents, 5.1% were discharged on triple therapy. Patients at highest risk of stroke (CHADS(2) score > or =2) were least likely to receive oral anticoagulation at discharge (39%). Warfarin use in patients with AF at discharge (43.4%) was associated with lower rates of 90 day mortality and stroke.
Conclusion: Atrial fibrillation prevalence at baseline and at discharge was 4.8 and 2.5%, respectively. The proportion of patients who developed new onset AF was 6.3%. New onset AF was independently associated with 90 day mortality and was a marker of adverse outcomes in patients undergoing primary PCI.
Figures
References
-
- Goldberg RJ, Seeley D, Becker RC, Brady P, Chen ZY, Osganian V, Gore JM, Alpert JS, Dalen JE. Impact of atrial fibrillation on the in-hospital and long-term survival of patients with acute myocardial infarction: a community-wide perspective. Am Heart J. 1990;119:996–1001. - PubMed
-
- Pedersen OD, Baggar H, Køber L, Torp-Perdersen C. The occurrence and prognostic significance of atrial fibrillation/-flutter following acute myocardial infarction. Eur Heart J. 1999;20:748–754. - PubMed
-
- Lopes RD, Pieper KS, Horton JR, Al-Khatib SM, Newby LK, Mehta RH, Van de Werf F, Armstrong PW, Mahaffey KW, Harrington RA, Ohman EM, White HD, Wallentin L, Granger CB. Short- and long-term outcomes following atrial fibrillation in patients with acute coronary syndromes with or without ST-segment elevation. Heart. 2008;94:867–873. - PubMed
-
- Crenshaw BS, Ward SR, Granger CB, Stebbins AL, Topol EJ, Califf RM. Atrial fibrillation in the setting of acute myocardial infarction: the GUSTO-I experience. J Am Coll Cardiol. 1997;30:406–413. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
