

A randomized trial of therapies for type 2 diabetes and coronary artery disease
- PMID: 19502645
- PMCID: PMC2863990
- DOI: 10.1056/NEJMoa0805796
A randomized trial of therapies for type 2 diabetes and coronary artery disease
Abstract
Background: Optimal treatment for patients with both type 2 diabetes mellitus and stable ischemic heart disease has not been established.
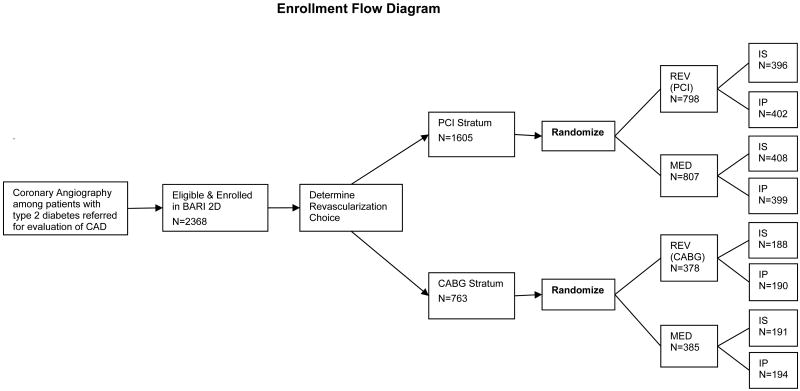
Methods: We randomly assigned 2368 patients with both type 2 diabetes and heart disease to undergo either prompt revascularization with intensive medical therapy or intensive medical therapy alone and to undergo either insulin-sensitization or insulin-provision therapy. Primary end points were the rate of death and a composite of death, myocardial infarction, or stroke (major cardiovascular events). Randomization was stratified according to the choice of percutaneous coronary intervention (PCI) or coronary-artery bypass grafting (CABG) as the more appropriate intervention.
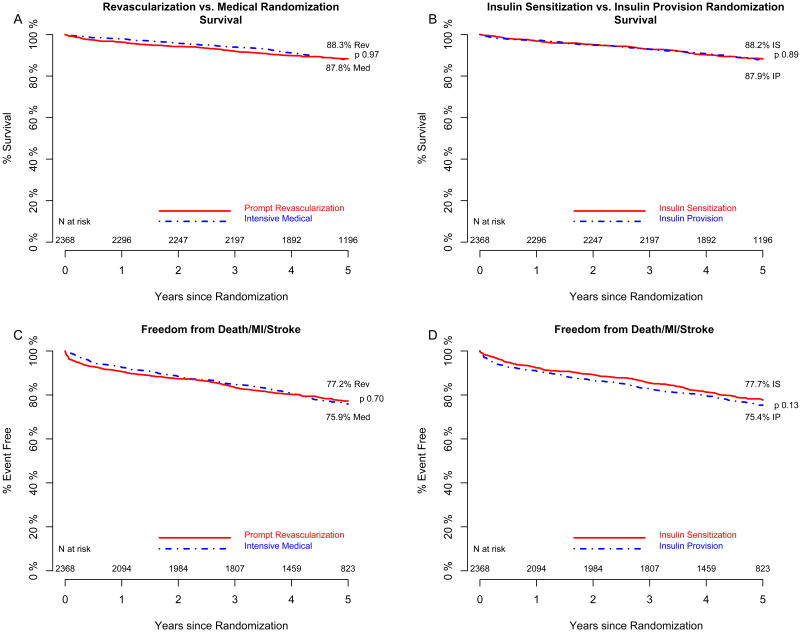
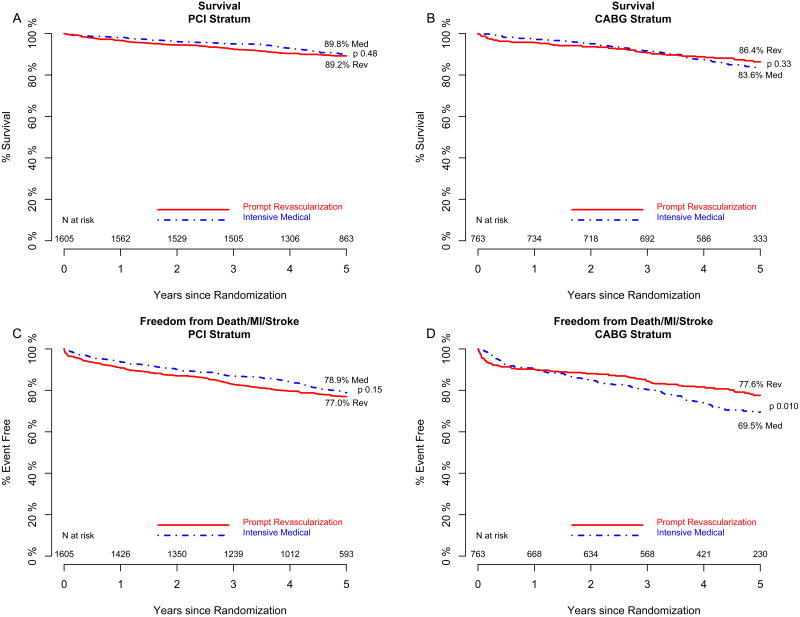
Results: At 5 years, rates of survival did not differ significantly between the revascularization group (88.3%) and the medical-therapy group (87.8%, P=0.97) or between the insulin-sensitization group (88.2%) and the insulin-provision group (87.9%, P=0.89). The rates of freedom from major cardiovascular events also did not differ significantly among the groups: 77.2% in the revascularization group and 75.9% in the medical-treatment group (P=0.70) and 77.7% in the insulin-sensitization group and 75.4% in the insulin-provision group (P=0.13). In the PCI stratum, there was no significant difference in primary end points between the revascularization group and the medical-therapy group. In the CABG stratum, the rate of major cardiovascular events was significantly lower in the revascularization group (22.4%) than in the medical-therapy group (30.5%, P=0.01; P=0.002 for interaction between stratum and study group). Adverse events and serious adverse events were generally similar among the groups, although severe hypoglycemia was more frequent in the insulin-provision group (9.2%) than in the insulin-sensitization group (5.9%, P=0.003).
Conclusions: Overall, there was no significant difference in the rates of death and major cardiovascular events between patients undergoing prompt revascularization and those undergoing medical therapy or between strategies of insulin sensitization and insulin provision. (ClinicalTrials.gov number, NCT00006305.)
2009 Massachusetts Medical Society
Conflict of interest statement
Dr. Frye reports serving on advisory boards for Sanofi-Aventis and Schering-Plough; Dr. Kelsey, serving on advisory boards for Sanofi-Aventis and Axio; Dr. Orchard, receiving consulting fees from AstraZeneca, Eli Lilly, and Takeda and grant support from VeraLight and having an equity interest in Bristol-Myers Squibb; Dr. Chaitman, receiving consulting fees from Eli Lilly and lecture fees from CV Therapeutics; Dr. Genuth, receiving consulting fees from Takeda, Sanofi-Aventis, and Merck; Dr. Hlatky, receiving consulting fees from Blue Cross Blue Shield Technology Evaluation Center and GE Healthcare and grant support from Aviir; Dr. Jones, having an equity interest in Amgen; Dr. Molitch, receiving consulting and lecture fees from Sanofi-Aventis and grant support from Amgen, Eli Lilly, Tercica, and Corcept Therapeutics; and Dr. Nesto, receiving consulting and lecture fees from GlaxoSmithKline and Sanofi-Aventis. No other potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Diabetes with coronary disease--a moving target amid evolving therapies?N Engl J Med. 2009 Jun 11;360(24):2570-2. doi: 10.1056/NEJMe0904090. Epub 2009 Jun 7. N Engl J Med. 2009. PMID: 19502646 No abstract available.
-
Therapies for type 2 diabetes and coronary artery disease.N Engl J Med. 2009 Oct 1;361(14):1407; author reply 1409-10. doi: 10.1056/NEJMc091419. N Engl J Med. 2009. PMID: 19797290 No abstract available.
-
Therapies for type 2 diabetes and coronary artery disease.N Engl J Med. 2009 Oct 1;361(14):1407-8; author reply 1409-10. N Engl J Med. 2009. PMID: 19802916 No abstract available.
-
Therapies for type 2 diabetes and coronary artery disease.N Engl J Med. 2009 Oct 1;361(14):1408; author reply 1409-10. N Engl J Med. 2009. PMID: 19802917 No abstract available.
-
Therapies for type 2 diabetes and coronary artery disease.N Engl J Med. 2009 Oct 1;361(14):1408-9; author reply 1409-10. N Engl J Med. 2009. PMID: 19802918 No abstract available.
-
ACP Journal Club. Adding prompt revascularization to medical therapy did not reduce mortality or CV events in patients with type 2 diabetes and CAD.Ann Intern Med. 2009 Oct 20;151(8):JC4-5. doi: 10.7326/0003-4819-151-8-200910200-02005. Ann Intern Med. 2009. PMID: 19841443 No abstract available.
-
[A randomized trial of therapies for type 2 diabetes and coronary artery disease].Kardiol Pol. 2009 Aug;67(8):932-4; discussion 935. Kardiol Pol. 2009. PMID: 19885988 Polish. No abstract available.
-
[Revascularization in patients with type 2 diabetes and coronary artery disease: BARI 2D (Bypass Angioplasty Revascularization Investigation 2 Diabetes) Study Group].Internist (Berl). 2010 May;51(5):674-6. doi: 10.1007/s00108-010-2593-6. Internist (Berl). 2010. PMID: 20352177 German. No abstract available.
References
-
- The Bypass Angioplasty Revascularization Investigation (BARI) Investigators. Comparison of coronary bypass surgery with angioplasty in patients with multivessel disease. N Engl J Med. 1996;335:217–225. Erratum, N Engl J Med 1997;336:147. - PubMed
-
- Geiss LS, Herman WH, Smith PJ. Mortality in non-insulin-dependent diabetes. In: Aubert RE, Ballard DJ, Barrett-Connor E, et al., editors. Diabetes in America (NIH publication no. 95-1468) 2nd. Bethesda, MD: National Institute of Diabetes and Digestive and Kidney Diseases; 1995. pp. 233–57.
-
- Mak KH, Moliterno DJ, Granger CB, et al. Influence of diabetes mellitus on clinical outcome in the thrombolytic era of acute myocardial infarction. J Am Coll Cardiol. 1997;30:171–179. - PubMed
-
- Malmberg K, Yusuf S, Gerstein HC, et al. Impact of diabetes on long-term prognosis in patients with unstable angina and non-Q-wave myocardial infarction: results of the OASIS (Organization to Assess Strategies for Ischemic Syndromes) Registry. Circulation. 2000;102:1014–1019. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous