

Bias associated with self-report of prior screening mammography
- PMID: 19505902
- PMCID: PMC2771779
- DOI: 10.1158/1055-9965.EPI-09-0020
Bias associated with self-report of prior screening mammography
Abstract
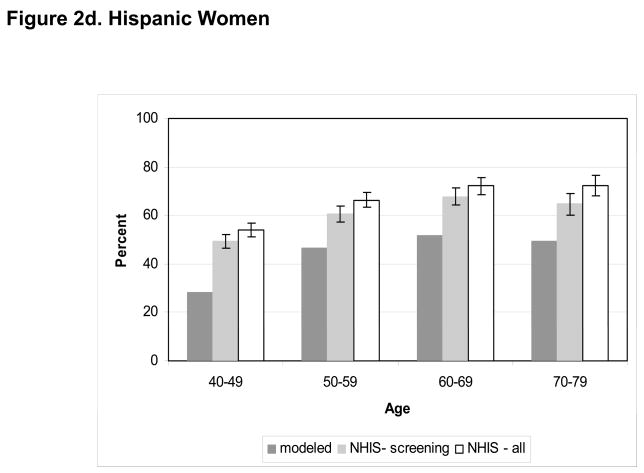
Background: Self-reported screening behaviors from national surveys often overestimate screening use, and the amount of overestimation may vary by demographic characteristics. We examine self-report bias in mammography screening rates overall, by age, and by race/ethnicity.
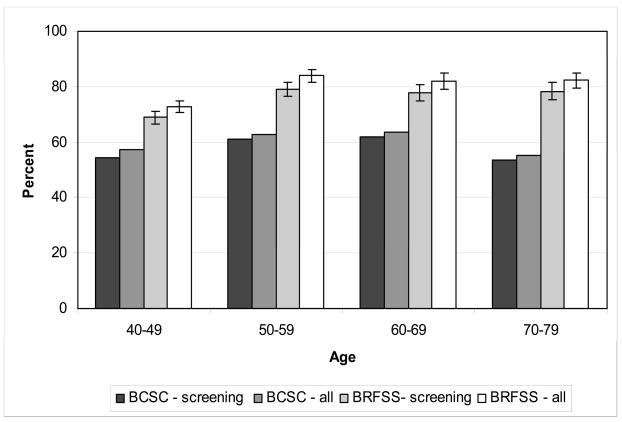
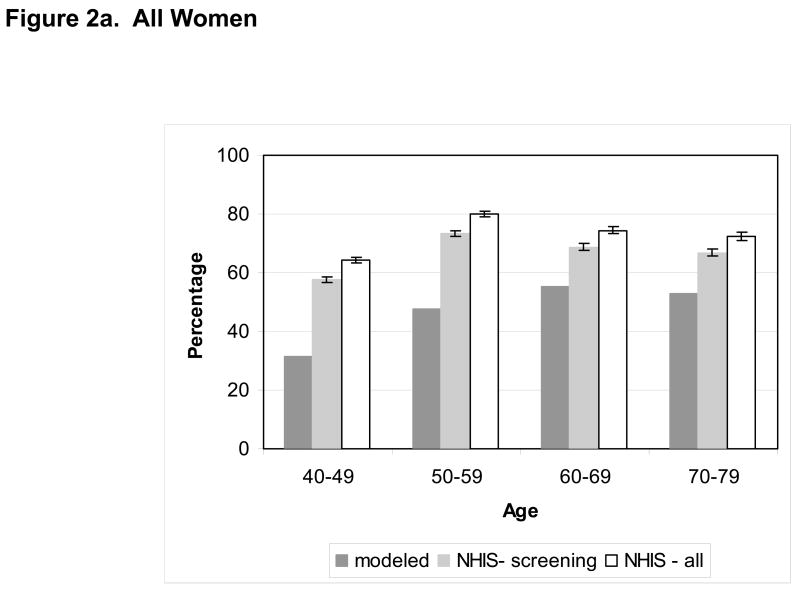
Methods: We use mammography registry data (1999-2000) from the Breast Cancer Surveillance Consortium to estimate the validity of self-reported mammography screening collected by two national surveys. First, we compare mammography use from 1999 to 2000 for a geographically defined population (Vermont) with self-reported rates in the prior two years from the 2000 Vermont Behavioral Risk Factor Surveillance System. We then use a screening dissemination simulation model to assess estimates of mammography screening from the 2000 National Health Interview Survey.
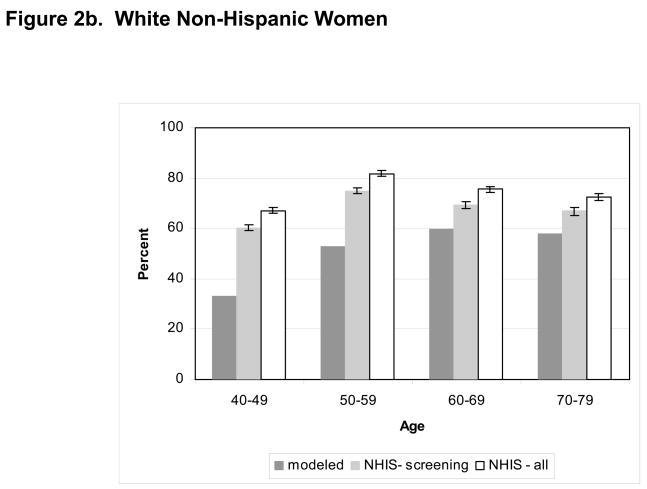
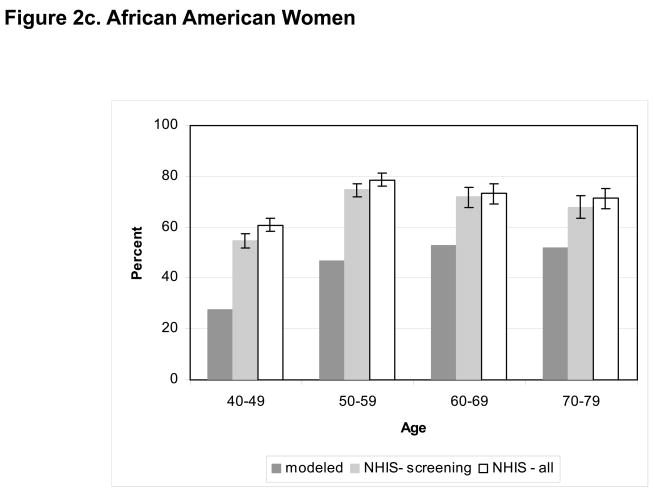
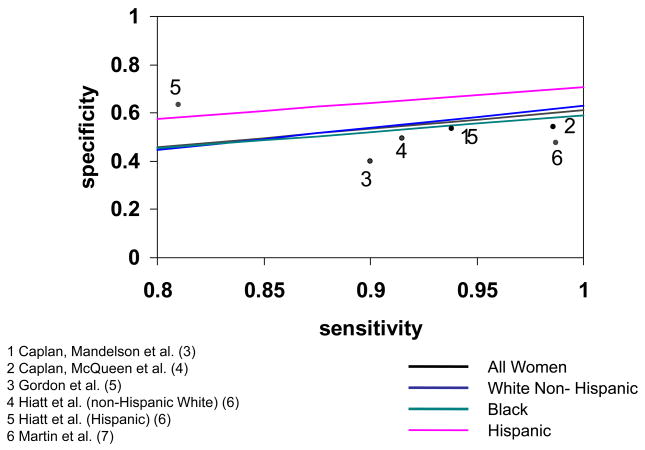
Results: Self-report estimates of mammography use in the prior 2 years from the Vermont Behavioral Risk Factor Surveillance System are 15 to 25 percentage points higher than actual screening rates across age groups. The differences in National Health Interview Survey screening estimates from models are similar for women 40 to 49 and 50 to 59 years and greater than for those 60 to 69, or 70 to 79 (27 and 26 percentage points versus 14, and 14, respectively). Overreporting is highest among African American women (24.4 percentage points) and lowest among Hispanic women (17.9) with non-Hispanic White women in between (19.3). Values of sensitivity and specificity consistent with our results are similar to previous validation studies of mammography.
Conclusion: Overestimation of self-reported mammography usage from national surveys varies by age and race/ethnicity. A more nuanced approach that accounts for demographic differences is needed when adjusting for overestimation or assessing disparities between populations.
Figures
References
-
- Newell SA, Girgis A, Sanson-Fisher RW, Savolainen NJ. The accuracy of self-reported health behaviors and risk factors relating to cancer and cardiovascular disease in the general population: A critical review. Am J Prev Med. 1999;17:211–29. - PubMed
-
- Rauscher GH, Johnson TP, Cho YI, Walk JA. Accuracy of Self-Reported Cancer-Screening Histories: A Meta-analysis. Cancer Epidemiol Biomarkers Prev. 2008;17:748–57. - PubMed
-
- Caplan LS, Mandelson MT, Anderson LA. Validity of Self-reported Mammography: Examining Recall and Covariates among Older Women in a Health Maintenance Organization. Am J Epidemiol. 2003;157:267–72. - PubMed
-
- Caplan LS, McQueen DV, Qualters JR, Leff M, Garrett C, Calonge N. Validity of Women’s Self-Reports of Cancer Screening Test Utilization in a Managed Care Population. Cancer Epidemiol Biomarkers Prev. 2003;12:1182–7. - PubMed
-
- Gordon NP, Hiatt RA, Lampert DI. Concordance of self-reported data and medical record audit for six cancer screening procedures. J Natl Cancer Inst. 1993;85:566–70. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 CA063740/CA/NCI NIH HHS/United States
- U01CA69976/CA/NCI NIH HHS/United States
- U01 CA070040/CA/NCI NIH HHS/United States
- U01CA70013/CA/NCI NIH HHS/United States
- U01 CA086082/CA/NCI NIH HHS/United States
- U01CA86082/CA/NCI NIH HHS/United States
- Z99 CA999999/ImNIH/Intramural NIH HHS/United States
- U01CA70040/CA/NCI NIH HHS/United States
- U01CA63740/CA/NCI NIH HHS/United States
- U01 CA063731/CA/NCI NIH HHS/United States
- U01 CA086076/CA/NCI NIH HHS/United States
- R55 NR004556/NR/NINR NIH HHS/United States
- U01CA63736/CA/NCI NIH HHS/United States
- U01 CA069976/CA/NCI NIH HHS/United States
- U01CA86076/CA/NCI NIH HHS/United States
- U01 CA063736/CA/NCI NIH HHS/United States
- U01 CA070013/CA/NCI NIH HHS/United States
- U01CA63731/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
