

Relation of disease pathogenesis and risk factors to heart failure with preserved or reduced ejection fraction: insights from the framingham heart study of the national heart, lung, and blood institute
- PMID: 19506115
- PMCID: PMC2775498
- DOI: 10.1161/CIRCULATIONAHA.108.815944
Relation of disease pathogenesis and risk factors to heart failure with preserved or reduced ejection fraction: insights from the framingham heart study of the national heart, lung, and blood institute
Abstract
Background: The contributions of risk factors and disease pathogenesis to heart failure with preserved ejection fraction (HFPEF) versus heart failure with reduced ejection fraction (HFREF) have not been fully explored.
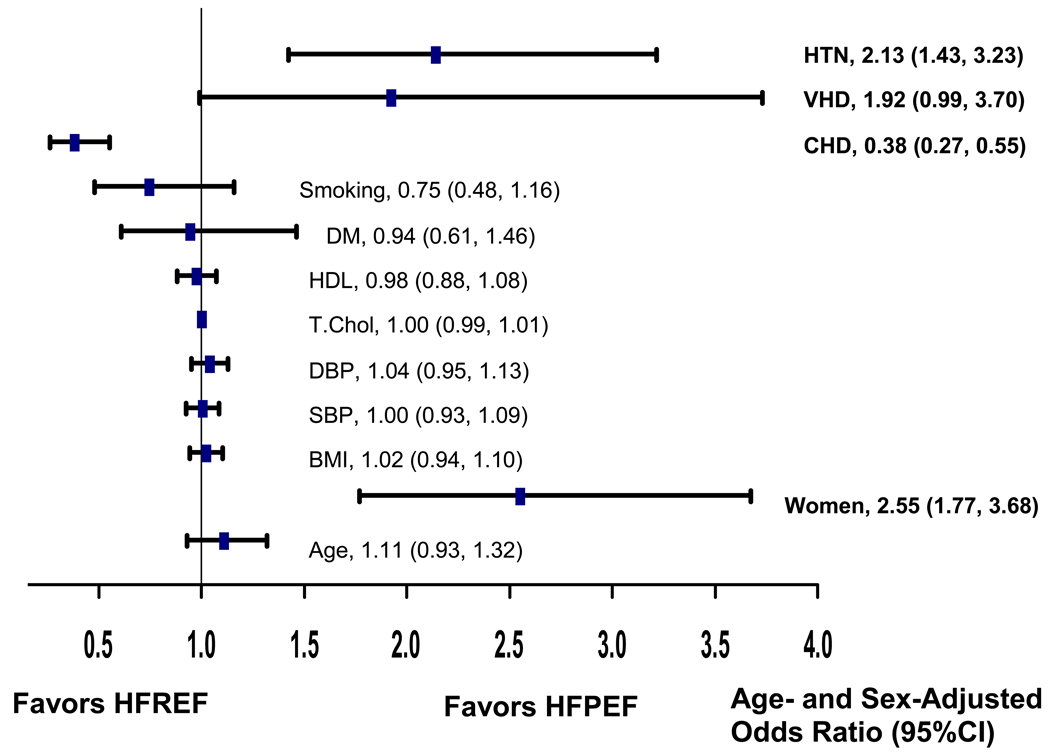
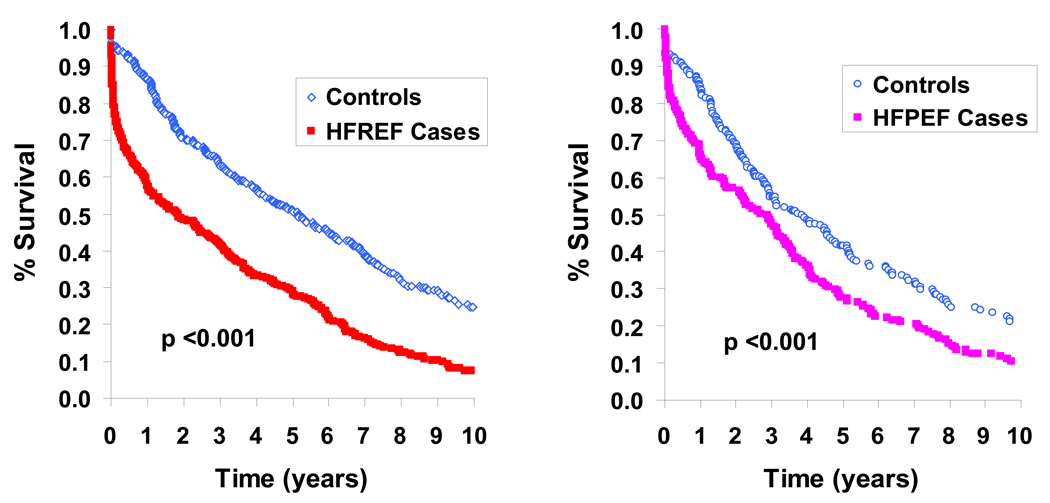
Methods and results: We examined clinical characteristics and risk factors at time of heart failure onset and long-term survival in Framingham Heart Study participants according to left ventricular ejection fraction < or =45% (n=314; 59%) versus >45% (n=220; 41%) and hierarchical causal classification. Heart failure was attributed to coronary heart disease in 278 participants (52%), valvular heart disease in 42 (8%), hypertension in 140 (26%), or other/unknown causes in 74 (14%). Multivariable predictors of HFPEF (versus HFREF) included elevated systolic blood pressure (odds ratio [OR]=1.13 per 10 mm Hg; 95% confidence interval [CI], 1.04 to 1.22), atrial fibrillation (OR=4.23; 95% CI, 2.38 to 7.52), and female sex (OR=2.29; 95% CI, 1.35 to 3.90). Conversely, prior myocardial infarction (OR=0.32; 95% CI, 0.19 to 0.53) and left bundle-branch block QRS morphology (OR=0.21; 95% CI, 0.10 to 0.46) reduced the odds of HFPEF. Long-term prognosis was grim, with a median survival of 2.1 years (5-year mortality rate, 74%), and was equally poor in men and women with HFREF or HFPEF.
Conclusions: Among community patients with new-onset heart failure, there are differences in causes and time-of-onset clinical characteristics between those with HFPEF versus HFREF. In people with HFREF, mortality is increased when coronary heart disease is the underlying cause. These findings suggest that heart failure with reduced left ventricular systolic function and heart failure with preserved left ventricular systolic function are partially distinct entities, with potentially different approaches to early detection and prevention.
Conflict of interest statement
No conflicts of interest to disclose.
Figures



Comment in
-
The heart failure spectrum: time for a phenotype-oriented approach.Circulation. 2009 Jun 23;119(24):3044-6. doi: 10.1161/CIRCULATIONAHA.109.870006. Epub 2009 Jun 8. Circulation. 2009. PMID: 19506105 No abstract available.
References
-
- Lee DS, Austin PC, Rouleau JL, Liu PP, Naimark D, Tu JV. Predicting mortality among patients hospitalized for heart failure: derivation and validation of a clinical model. JAMA. 2003;290:2581–2587. - PubMed
-
- Lee DS, Tu JV, Juurlink DN, Alter DA, Ko DT, Austin PC, Chong A, Stukel TA, Levy D, Laupacis A. Risk-treatment mismatch in the pharmacotherapy of heart failure. JAMA. 2005;294:1240–1247. - PubMed
-
- Vasan RS, Larson MG, Benjamin EJ, Evans JC, Reiss CK, Levy D. Congestive heart failure in subjects with normal versus reduced left ventricular ejection fraction: prevalence and mortality in a population- based cohort. J Am Coll Cardiol. 1999;33:1948–1955. - PubMed
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355:251–259. - PubMed
-
- Ho KK, Anderson KM, Kannel WB, Grossman W, Levy D. Survival after the onset of congestive heart failure in Framingham Heart Study subjects. Circulation. 1993;88:107–115. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
