

Primary therapy of Waldenström macroglobulinemia with bortezomib, dexamethasone, and rituximab: WMCTG clinical trial 05-180
- PMID: 19506160
- PMCID: PMC2727288
- DOI: 10.1200/JCO.2008.20.4677
Primary therapy of Waldenström macroglobulinemia with bortezomib, dexamethasone, and rituximab: WMCTG clinical trial 05-180
Abstract
Purpose: We examined the activity of bortezomib, dexamethasone, and rituximab (BDR) in patients with symptomatic, untreated Waldenström macroglobulinemia (WM).
Patients and methods: A cycle of therapy consisted of bortezomib 1.3 mg/m(2) intravenously; dexamethasone 40 mg on days 1, 4, 8, and 11; and rituximab 375 mg/m(2) on day 11. Patients received four consecutive cycles for induction therapy and then four more cycles, each given 3 months apart, for maintenance therapy. Twenty-three patients received a median of seven cycles of treatment.
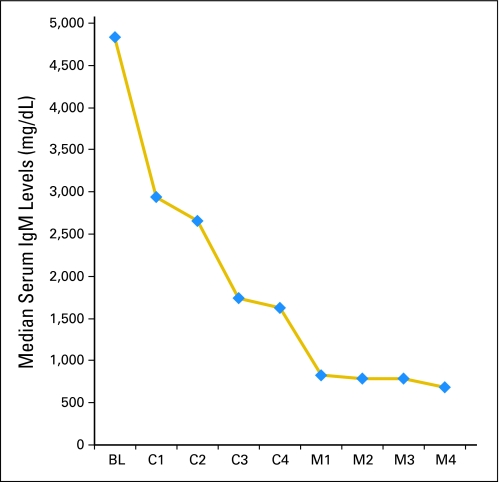
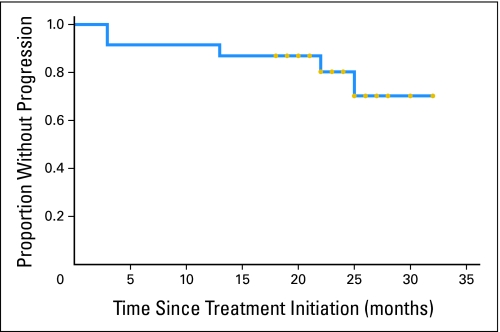
Results: Median bone marrow disease involvement declined from 55% to 10% (P = .0004), serum immunoglobulin M levels declined from 4,830 to 1,115 mg/dL (P < .0001), and hematocrit increased from 29.8% to 38.2% (P = .0002) at best response. The overall response rates and major response rates were 96% and 83% with three complete responses, two near complete responses, three very good partial responses, 11 partial responses, and three minor responses. Responses occurred at a median of 1.4 months. With a median follow-up of 22.8 months, 18 of 23 patients remained free of disease progression. Peripheral neuropathy was the most common toxicity, and it resolved to grade < or = 1 in 13 of 16 patients at a median of 6.0 months. Four of the first seven treated patients developed herpes zoster, resulting in the institution of prophylactic antiviral therapy.
Conclusion: The results demonstrate that BDR produces rapid and durable responses, along with high rates of response and complete remissions in WM. Herpes zoster prophylaxis is necessary with BDR, and reversible peripheral neuropathy was the most common toxicity leading to premature discontinuation of bortezomib in 61% of patients. Exploration of alternative schedules for bortezomib administration that includes weekly dosing should be pursued.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Owen RG, Treon SP, Al-Katib A, et al. Clinicopathological definition of Waldenström's macroglobulinemia: Consensus panel recommendations from the Second International Workshop on Waldenström's Macroglobulinemia. Semin Oncol. 2003;30:110–115. - PubMed
-
- Harris NL, Jaffe ES, Stein H. A revised European-American classification of lymphoid neoplasms: A proposal from the International Lymphoma Study Group. Blood. 1994;84:1361–1392. - PubMed
-
- Harris NL, Jaffe ES, Diebold J, et al. World Health Organization classification of neoplastic diseases of the hematopoietic and lymphoid tissues: Report of the Clinical Advisory Committee meeting-Airlie House, Virginia, November 1997. J Clin Oncol. 1999;17:3835–3849. - PubMed
-
- Treon SP, Hunter ZR, Aggarwal A, et al. Characterization of familial Waldenstrom's macroglobulinemia. Ann Oncol. 2006;17:488–494. - PubMed
-
- Mitsiades CS, Mitsiades N, Richardson PG, et al. Novel biologically based therapies for Waldenstrom's macroglobulinemia. Semin Oncol. 2003;30:309–312. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
