

In-hospital case fatality rates for acute myocardial infarction in Romania
- PMID: 19506280
- PMCID: PMC2691436
- DOI: 10.1503/cmaj.081227
In-hospital case fatality rates for acute myocardial infarction in Romania
Abstract
Background: We describe the clinical characteristics, treatments and in-hospital case-fatality rates in an unselected population of patients admitted for acute myocardial infarction.
Methods: From January 2000 to June 2007, we tracked consecutive patients who were admitted to 7 tertiary referral and 21 county hospitals in Romania for medical treatment of ST-segment elevation acute myocardial infarction. These patients were enrolled in the Romanian Registry for ST-segment Elevation Myocardial Infarction. For this prospective study, we collected data on demographic characteristics, cardiovascular risk factors, various aspects of treatment for myocardial infarction, and in-hospital death.
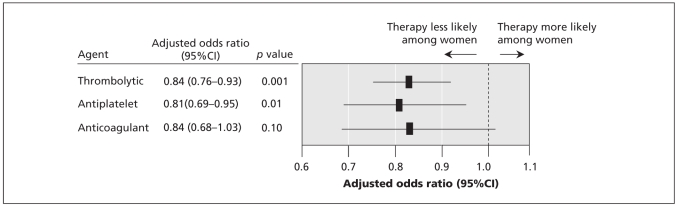
Results: The 9186 patients in the study group had a mean age of 63.8 years. The median time from onset of symptoms to thrombolysis was 230 (interquartile range 120-510) minutes. Of the 9186 patients, 4986 (54.3%) had hypertension, 1974 (21.5%) had diabetes mellitus, 3545 (38.6%) had lipid disorders and 4653 (50.7%) were smokers. The in-hospital mortality rate was 12.7% (1170 deaths). The study group consisted of 2893 women and 6293 men. The women were older than the men and had higher rates of hypertension and diabetes mellitus but were less likely to be smokers. A smaller proportion of women than men presented within 2 hours after onset of symptoms (23.1% v. 34.4%, p < 0.001). Smaller proportions of women received thrombolytics (40.8% v. 53.5%, p < 0.001), anticoagulants (93.4% v. 95.2%; p = 0.001), antiplatelet agents (88.3% v. 91.2%, p < 0.001) and primary percutaneous coronary interventions (1.5% v. 2.2%, p = 0.030). The risk of in-hospital death was greater for women, even after adjustment for confounders (odds ratio 1.33, 95% confidence interval 1.13-1.56; p < 0.001).
Interpretation: The rates of reperfusion therapy for patients with acute myocardial infarction were low, and in-hospital case-fatality rates were high in this study. Excess in-hospital mortality was more pronounced among women.
Figures
Comment in
-
Quality of acute coronary care in emerging economies.CMAJ. 2009 Jun 9;180(12):1190-1. doi: 10.1503/cmaj.090503. CMAJ. 2009. PMID: 19506274 Free PMC article. No abstract available.
References
-
- World Health Organization, Regional Office for Europe. The European health report 2002. Copenhagen (Denmark): The Organization; 2002. pp. 7–45.
-
- Tunstall-Pedoe H, Vanuzzo D, Hobbs M, et al. Estimation of contribution of changes in coronary care to improving survival, event rates, and coronary heart disease mortality across the WHO MONICA project populations. Lancet. 2000;355:688–700. - PubMed
-
- U.S. government assistance to Eastern Europe under the Support for East European Democracy (SEED) Act. Washington (DC): US Department of State, Bureau of European and Eurasian Affairs; 2004. pp. 68–113.
-
- Gurjeva OS, Bukhman G, Murphy S, et al. Treatment and outcomes of eastern Europeans with coronary syndromes in OPUS-TIMI 16. Int J Cardiol. 2005;100:101–7. - PubMed
-
- Kramer JM, Newby LK, Chang WC, et al. International variation in the use of evidence-based medicines for acute coronary syndromes. Eur Heart J. 2003;24:2133–41. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical