

Static platelet adhesion, flow cytometry and serum TXB2 levels for monitoring platelet inhibiting treatment with ASA and clopidogrel in coronary artery disease: a randomised cross-over study
- PMID: 19508722
- PMCID: PMC2699331
- DOI: 10.1186/1479-5876-7-42
Static platelet adhesion, flow cytometry and serum TXB2 levels for monitoring platelet inhibiting treatment with ASA and clopidogrel in coronary artery disease: a randomised cross-over study
Abstract
Background: Despite the use of anti-platelet agents such as acetylsalicylic acid (ASA) and clopidogrel in coronary heart disease, some patients continue to suffer from atherothrombosis. This has stimulated development of platelet function assays to monitor treatment effects. However, it is still not recommended to change treatment based on results from platelet function assays. This study aimed to evaluate the capacity of a static platelet adhesion assay to detect platelet inhibiting effects of ASA and clopidogrel. The adhesion assay measures several aspects of platelet adhesion simultaneously, which increases the probability of finding conditions sensitive for anti-platelet treatment.
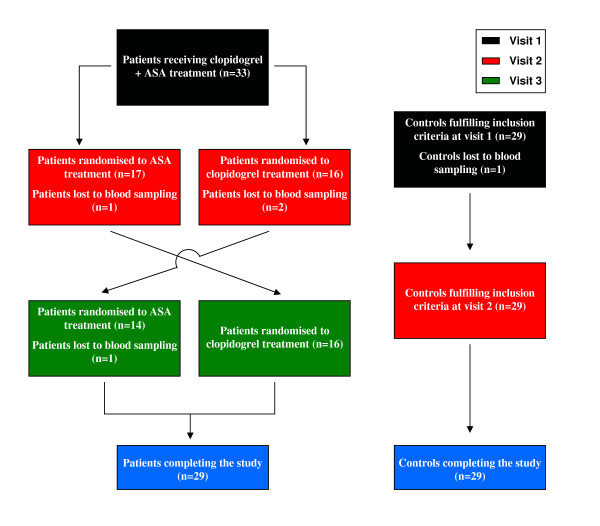
Methods: With a randomised cross-over design we evaluated the anti-platelet effects of ASA combined with clopidogrel as well as monotherapy with either drug alone in 29 patients with a recent acute coronary syndrome. Also, 29 matched healthy controls were included to evaluate intra-individual variability over time. Platelet function was measured by flow cytometry, serum thromboxane B2 (TXB2)-levels and by static platelet adhesion to different protein surfaces. The results were subjected to Principal Component Analysis followed by ANOVA, t-tests and linear regression analysis.
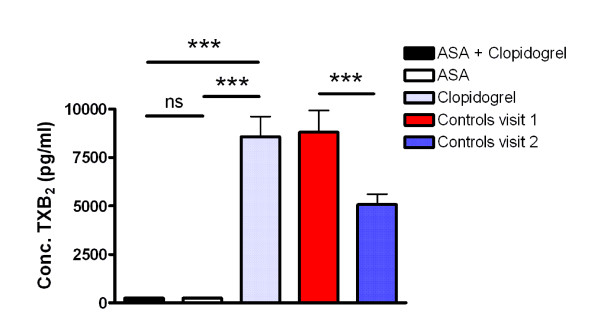
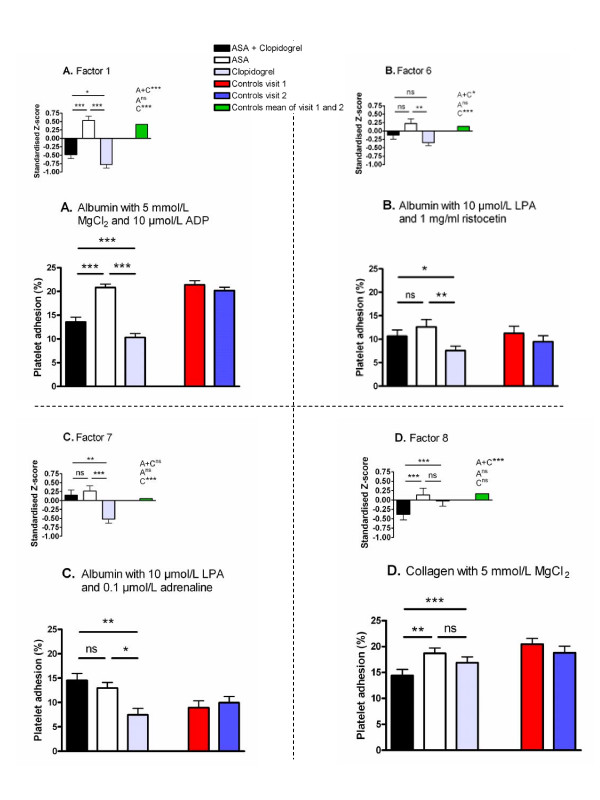
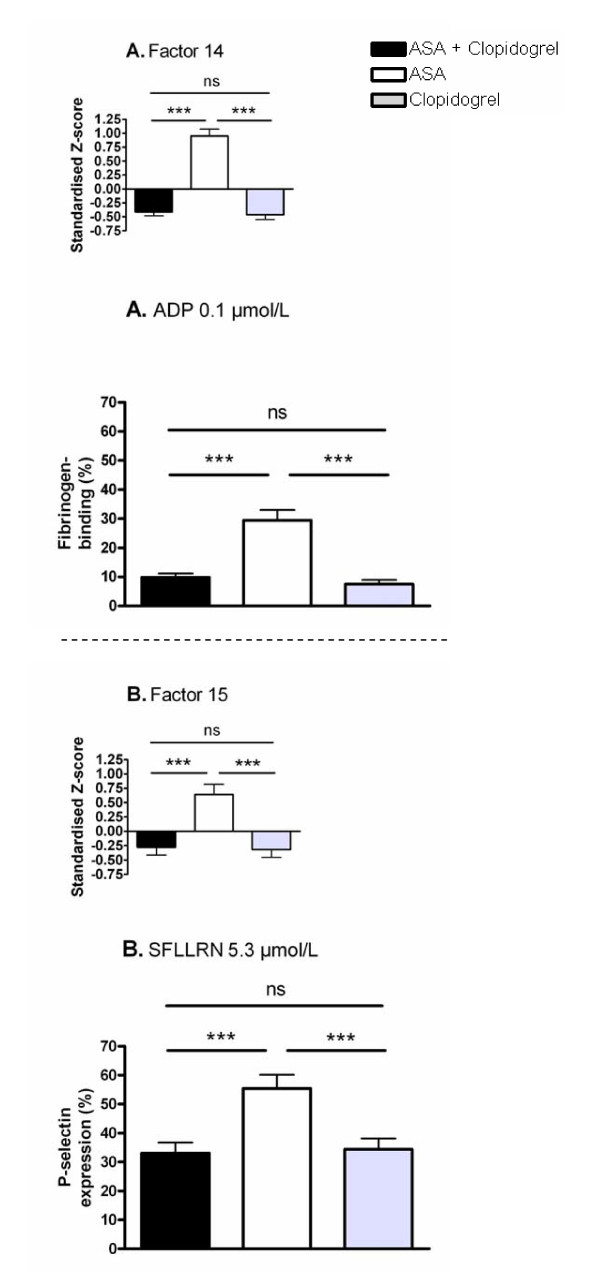
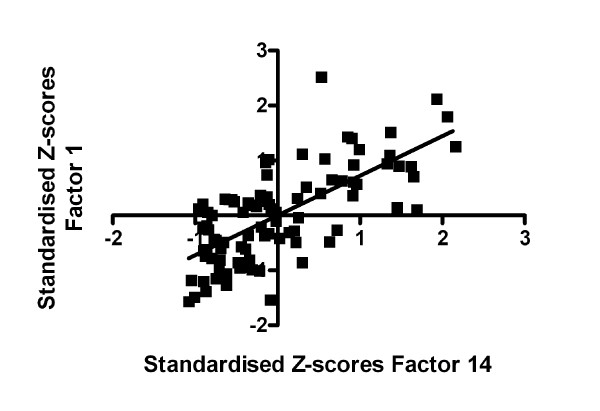
Results: The majority of platelet adhesion measures were reproducible in controls over time denoting that the assay can monitor platelet activity. Adenosine 5'-diphosphate (ADP)-induced platelet adhesion decreased significantly upon treatment with clopidogrel compared to ASA. Flow cytometric measurements showed the same pattern (r2 = 0.49). In opposite, TXB2-levels decreased with ASA compared to clopidogrel. Serum TXB2 and ADP-induced platelet activation could both be regarded as direct measures of the pharmacodynamic effects of ASA and clopidogrel respectively. Indirect pharmacodynamic measures such as adhesion to albumin induced by various soluble activators as well as SFLLRN-induced activation measured by flow cytometry were lower for clopidogrel compared to ASA. Furthermore, adhesion to collagen was lower for ASA and clopidogrel combined compared with either drug alone.
Conclusion: The indirect pharmacodynamic measures of the effects of ASA and clopidogrel might be used together with ADP-induced activation and serum TXB2 for evaluation of anti-platelet treatment. This should be further evaluated in future clinical studies where screening opportunities with the adhesion assay will be optimised towards increased sensitivity to anti-platelet treatment.
Figures
References
-
- Sabatine MS, Cannon CP, Gibson CM, Lopez-Sendon JL, Montalescot G, Theroux P, Claeys MJ, Cools F, Hill KA, Skene AM, McCabe CH, Braunwald E. Addition of clopidogrel to aspirin and fibrinolytic therapy for myocardial infarction with ST-segment elevation. N Engl J Med. 2005;352:1179–1189. doi: 10.1056/NEJMoa050522. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
