

Side matters: diffusion tensor imaging tractography in left and right temporal lobe epilepsy
- PMID: 19509072
- PMCID: PMC2759860
- DOI: 10.3174/ajnr.A1650
Side matters: diffusion tensor imaging tractography in left and right temporal lobe epilepsy
Abstract
Background and purpose: Noninvasive imaging plays a pivotal role in lateralization of the seizure focus in presurgical patients with temporal lobe epilepsy (TLE). Our goal was to evaluate the utility of diffusion tensor imaging (DTI) tractography in TLE.
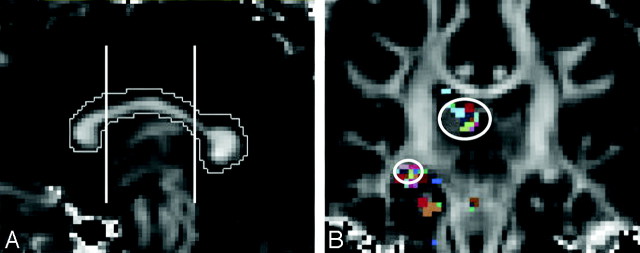
Materials and methods: Twenty-one patients with TLE (11 right, 10 left TLE) and 21 controls were enrolled. A 1.5T MR imaging scanner was used to obtain 51 diffusion-gradient-direction images per subject. Eight pairs of white matter fiber tracts were traced, and fiber tract fractional anisotropy (FA) was calculated and compared with controls. Fiber tract FA asymmetry and discriminant function analysis were evaluated in all subjects and fiber tracts respectively.
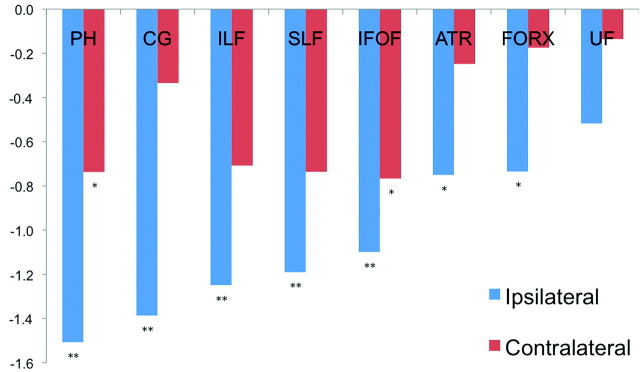
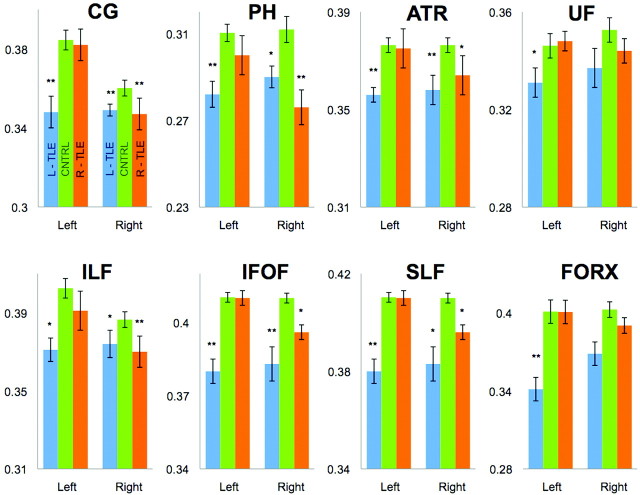
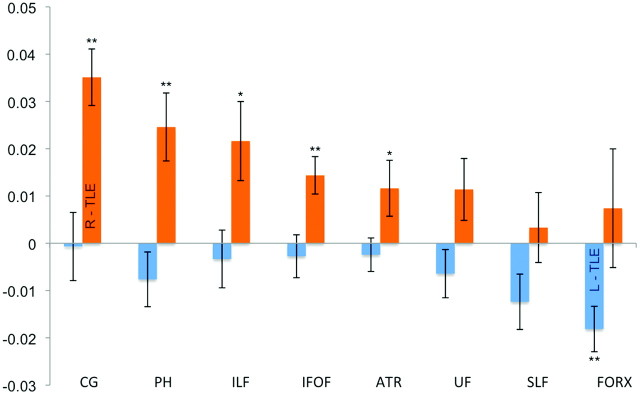
Results: Compared with controls, patients with TLE demonstrated decreased FA in 5 ipsilateral fiber tracts. Patients with left TLE had 6 ipsilateral and 4 contralateral fiber tracts with decreased FA. Patients with right TLE had 4 ipsilateral but no contralateral tracts with decreased FA compared with controls. Right-sided FA asymmetry was demonstrated in patients with right TLE for 5 fiber tracts, and left-sided asymmetry, for patients with left TLE for 1 fiber tract. Discriminant function analysis correctly categorized patients into left-versus-right TLE in 90% of all cases (100% correct in all patients without hippocampal sclerosis) by using uncinate fasciculus and parahippocampal fiber tracts.
Conclusions: We found widespread reductions in fiber tract FA in patients with TLE, which were most pronounced ipsilateral to the seizure focus. Patients with left TLE had greater, more diffuse changes, whereas patients with right TLE showed changes that were primarily ipsilateral. Disease was lateralized to a high degree independent of identifiable hippocampal pathology noted on conventional MR imaging.
Figures

References
-
- Hirtz D, Thurman DJ, Gwinn-Hardy K, et al. How common are the “common” neurologic disorders? Neurology 2007;68:326–37 - PubMed
-
- Hauser WA, Annegers JF, Kurland LT. Prevalence of epilepsy in Rochester, Minnesota: 1940–80. Epilepsia 1991;32:429–45 - PubMed
-
- Engel J., Jr Mesial temporal lobe epilepsy: what have we learned? Neuroscientist 2001;7:340–52 - PubMed
-
- McIntosh AM, Kalnins RM, Mitchell LA, et al. Temporal lobectomy: long-term seizure outcome, late recurrence and risks for seizure recurrence. Brain 2004;127:2018–30 - PubMed
-
- Juhasz C, Chugani HT. Imaging the epileptic brain with positron emission tomography. Neuroimaging Clin N Am 2003;13:705–16, viii - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources