

Coapplication of lidocaine and the permanently charged sodium channel blocker QX-314 produces a long-lasting nociceptive blockade in rodents
- PMID: 19512868
- PMCID: PMC2761747
- DOI: 10.1097/ALN.0b013e3181a915e7
Coapplication of lidocaine and the permanently charged sodium channel blocker QX-314 produces a long-lasting nociceptive blockade in rodents
Abstract
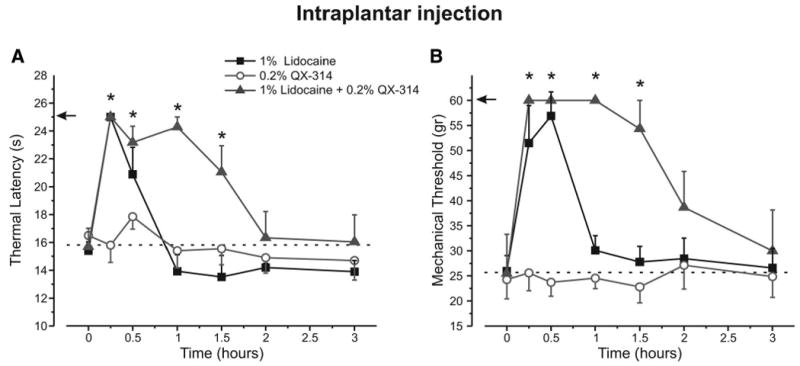
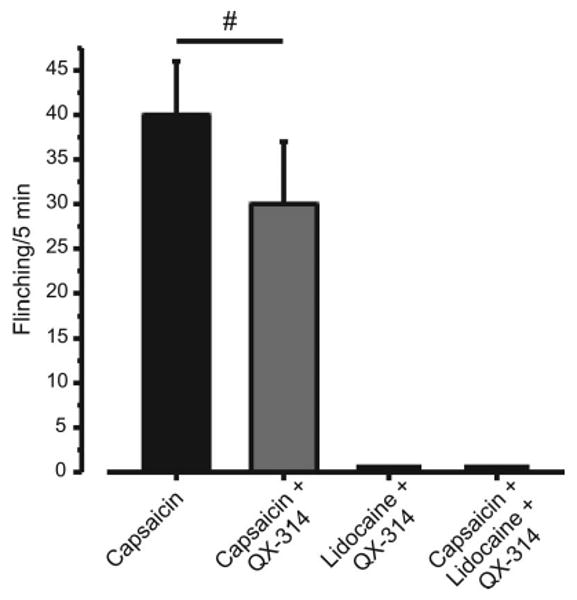
Background: Nociceptive-selective local anesthesia is produced by entry of the permanently charged lidocaine-derivative QX-314 into nociceptors when coadministered with capsaicin, a transient receptor potential vanilloid 1 (TRPV1) channel agonist. However, the pain evoked by capsaicin before establishment of the QX-314-mediated block would limit clinical utility. Because TRPV1 channels are also activated by lidocaine, the authors tested whether lidocaine can substitute for capsaicin to introduce QX-314 into nociceptors through TRPV1 channels and produce selective analgesia.
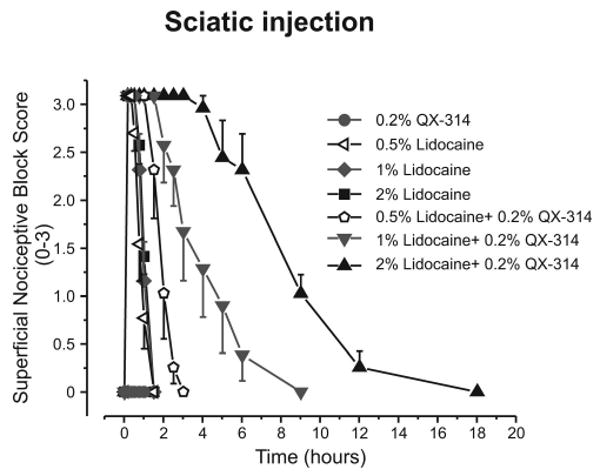
Methods: Lidocaine (0.5% [17.5 mM], 1% [35 mM], and 2% [70 mM]) alone, QX-314 (0.2% [5.8 mM]) alone, and a combination of the two were injected subcutaneously and adjacent to the sciatic nerve in rats and mice. Mechanical and thermal responsiveness were measured, as was motor block.
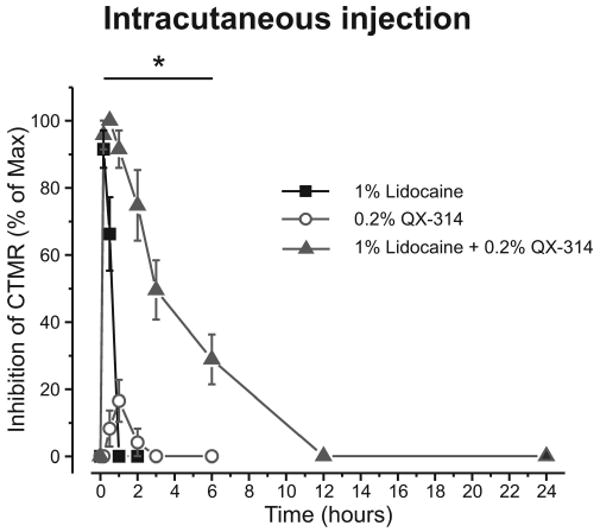
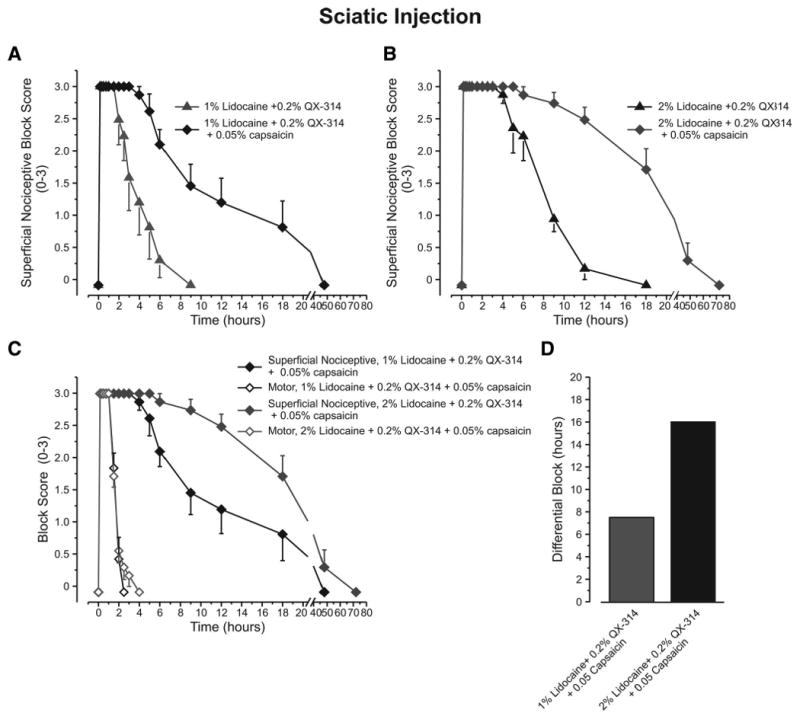
Results: Coapplication of 0.2% QX-314 with lidocaine prolonged the nociceptive block relative to lidocaine alone, an effect attenuated in TRPV1 knockout mice. The 0.2% QX-314 alone had no effect when injected intraplantary or perineurally, and it produced only weak short-lasting inhibition of the cutaneous trunci muscle reflex. Perisciatic nerve injection of lidocaine with QX-314 produced a differential nociceptive block much longer than the transient motor block, lasting 2 h (for 1% lidocaine) to 9 h (2% lidocaine). Triple application of lidocaine, QX-314, and capsaicin further increased the duration of the differential block.
Conclusions: Coapplication of lidocaine and its quaternary derivative QX-314 produces a long-lasting, predominantly nociceptor-selective block, likely by facilitating QX-314 entry through TRPV1 channels. Delivery of QX-314 into nociceptors by using lidocaine instead of capsaicin produces sustained regional analgesia without nocifensive behavior.
Figures


Comment in
-
Local anesthetics: a new hydrophilic pathway for the drug-receptor reaction.Anesthesiology. 2009 Jul;111(1):12-4. doi: 10.1097/ALN.0b013e3181a91624. Anesthesiology. 2009. PMID: 19512864 No abstract available.
References
-
- Binshtok AM, Bean BP, Woolf CJ. Inhibition of nociceptors by TRPV1-mediated entry of impermeant sodium channel blockers. Nature. 2007;449:607–10. - PubMed
-
- Amaya F, Wang H, Costigan M, Allchorne AJ, Hatcher JP, Egerton J, Stean T, Morisset V, Grose D, Gunthorpe MJ, Chessell IP, Tate S, Green PJ, Woolf CJ. The voltage-gated sodium channel Na (v) 1.9 is an effector of peripheral inflammatory pain hypersensitivity. J Neurosci. 2006;26:12852–60. - PMC - PubMed
-
- Hargreaves K, Dubner R, Brown F, Flores C, Joris J. A new and sensitive method for measuring thermal nociception in cutaneous hyperalgesia. Pain. 1988;32:77–88. - PubMed
-
- Thalhammer JG, Vladimirova M, Bershadsky B, Strichartz GR. Neurologic evaluation of the rat during sciatic nerve block with lidocaine. Anesthesiology. 1995;82:1013–25. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
