

Erectile function recovery rate after radical prostatectomy: a meta-analysis
- PMID: 19515209
- PMCID: PMC4097184
- DOI: 10.1111/j.1743-6109.2009.01351.x
Erectile function recovery rate after radical prostatectomy: a meta-analysis
Abstract
Introduction: Erectile function recovery (EFR) rates after radical prostatectomy (RP) vary greatly based on a number of factors, such as erectile dysfunction (ED) definition, data acquisition means, time-point postsurgery, and population studied.
Aim: To conduct a meta-analysis of carefully selected reports from the available literature to define the EFR rate post-RP.
Main outcome measures: EFR rate after RP.
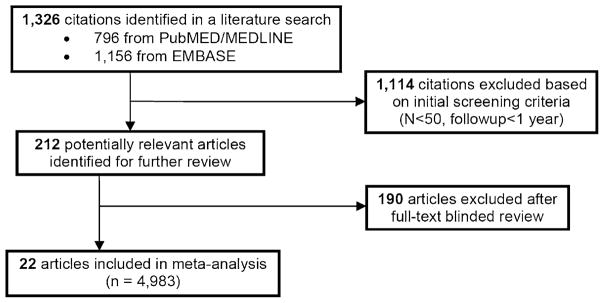
Methods: An EMBASE and MEDLINE search was conducted for the time range 1985-2007. Articles were assessed blindly by strict inclusion criteria: report of EFR data post-RP, study population >or=50 patients, >or=1 year follow-up, nerve-sparing status declared, no presurgery ED, and no other prostate cancer therapy. Meta-analysis was conducted to determine the EFR rate and relative risks (RR) for dichotomous subgroups.
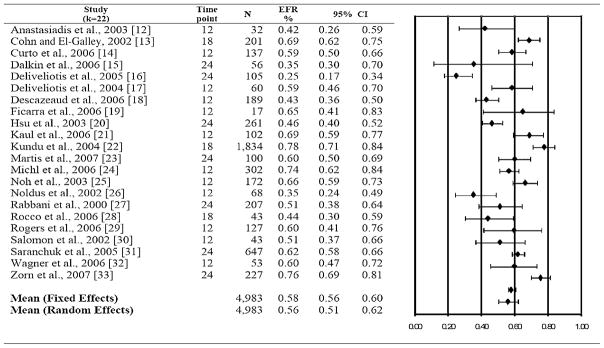
Results: A total of 212 relevant studies were identified; only 22 (10%) met the inclusion criteria and were analyzed (9,965 RPs, EFR data: 4,983 subjects). Mean study population size: 226.5, standard deviation = 384.1 (range: 17-1,834). Overall EFR rate was 58%. Single center series publications (k = 19) reported a higher EFR rate compared with multicenter series publications (k = 3): 60% vs. 33%, RR = 1.82, P = 0.001. Studies reporting >or=18-month follow-up (k = 10) reported higher EFR rate vs. studies with <18-month follow-up (k = 12), 60% vs. 56%, RR = 1.07, P = 0.02. Open RP (k = 16) and laparoscopic RP (k = 4) had similar EFR (57% vs. 58%), while robot-assisted RP resulted in a higher EFR rate (k = 2), 73% compared with these other approaches, P = 0.001. Patients <60 years old had a higher EFR rate vs. patients >or=60 years, 77% vs. 61%, RR = 1.26, P = 0.001.
Conclusions: These data indicate that most of the published literature does not meet strict criteria for reporting post-RP EFR. Single and multiple surgeon series have comparable EFR rates, but single center studies have a higher EFR. Younger men have higher EFR and no significant difference in EFR between ORP and LRP is evident.
Conflict of interest statement
Figures
References
-
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, Thun MJ. Cancer statistics, 2008. CA Cancer J Clin. 2008;58:71–96. - PubMed
-
- Bill-Axelson A, Holmberg L, Ruutu M, Haggman M, Andersson SO, Bratell S, Spangberg A, Busch C, Nordling S, Garmo H, Palmgren J, Adami HO, Norlen BJ, Johansson JE. Radical prostatectomy versus watchful waiting in early prostate cancer. N Engl J Med. 2005;352:1977–84. - PubMed
-
- Walsh PC, Donker PJ. Impotence following radical prostatectomy: insight into etiology and prevention. J Urol. 1982;128:492–7. - PubMed
-
- Sanchez-Cruz JJ, Cabrera-Leon A, Martin-Morales A, Fernandez A, Burgos R, Rejas J. Male erectile dysfunction and health-related quality of life. Eur Urol. 2003;44:245–53. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
