

Pilot study of Lokomat versus manual-assisted treadmill training for locomotor recovery post-stroke
- PMID: 19523207
- PMCID: PMC2708184
- DOI: 10.1186/1743-0003-6-18
Pilot study of Lokomat versus manual-assisted treadmill training for locomotor recovery post-stroke
Abstract
Background: While manually-assisted body-weight supported treadmill training (BWSTT) has revealed improved locomotor function in persons with post-stroke hemiparesis, outcomes are inconsistent and it is very labor intensive. Thus an alternate treatment approach is desirable. Objectives of this pilot study were to: 1) compare the efficacy of body-weight supported treadmill training (BWSTT) combined with the Lokomat robotic gait orthosis versus manually-assisted BWSTT for locomotor training post-stroke, and 2) assess effects of fast versus slow treadmill training speed.
Methods: Sixteen volunteers with chronic hemiparetic gait (0.62 +/- 0.30 m/s) post-stroke were randomly allocated to Lokomat (n = 8) or manual-BWSTT (n = 8) 3x/wk for 4 weeks. Groups were also stratified by fast (mean 0.92 +/- 0.15 m/s) or slow (0.58 +/- 0.12 m/s) training speeds. The primary outcomes were self-selected overground walking speed and paretic step length ratio. Secondary outcomes included: fast overground walking speed, 6-minute walk test, and a battery of clinical measures.
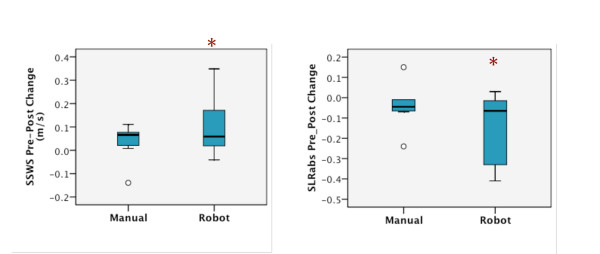
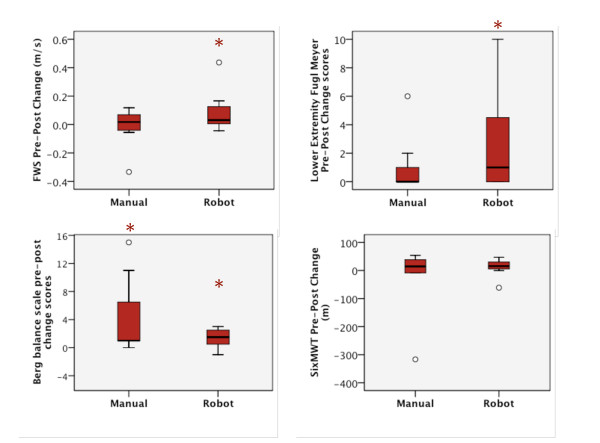
Results: No significant differences in primary outcomes were revealed between Lokomat and manual groups as a result of training. However, within the Lokomat group, self-selected walk speed, paretic step length ratio, and four of the six secondary measures improved (p = 0.04-0.05, effect sizes = 0.19-0.60). Within the manual group, only balance scores improved (p = 0.02, effect size = 0.57). Group differences between fast and slow training groups were not revealed (p > or = 0.28).
Conclusion: Results suggest that Lokomat training may have advantages over manual-BWSTT following a modest intervention dose in chronic hemiparetic persons and further, that our training speeds produce similar gait improvements. Suggestions for a larger randomized controlled trial with optimal study parameters are provided.
Figures
References
-
- Perry J, Garrett M, Gronley JK, Mulroy SJ. Classification of walking handicap in the stroke population. Stroke. 1995;26:982–989. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
