

Synchronous primary carcinoid tumor and primary adenocarcinoma arising within mature cystic teratoma of horseshoe kidney: a unique case report and review of the literature
- PMID: 19523243
- PMCID: PMC2704177
- DOI: 10.1186/1746-1596-4-17
Synchronous primary carcinoid tumor and primary adenocarcinoma arising within mature cystic teratoma of horseshoe kidney: a unique case report and review of the literature
Abstract
Background: Malignant transformation of mature cystic teratoma is a rare complication. While any of the constituent tissues of a teratoma has the potential to undergo malignant transformation, squamous cell carcinoma is the most commonly associated malignancy. Renal carcinoid tumors are rare and frequently associated with horseshoe kidney and renal teratoma. Renal teratoma rarely presents together with carcinoid tumor or adenocarcinoma. To the best of our knowledge, there has never been a report of renal teratoma coexisting with both carcinoid tumor and adenocarcinoma.
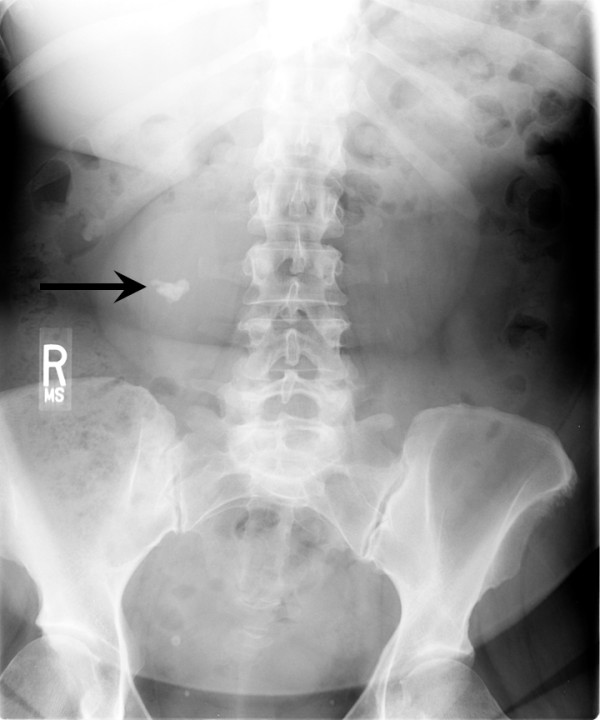
Methods: Here, we present a unique and first case of synchronous primary carcinoid tumor and moderately differentiated adenocarcinoma arising within mature cystic teratoma of horseshoe kidney in a 50-year-old female. Lumbar spine X-ray, done for her complaint of progressive chronic low back pain, accidentally found a large calcification overlying the lower pole of the right kidney. Further radiologic studies revealed horseshoe kidney and a large multi-septated cystic lesion immediately anterior to the right renal pelvis with central calcification and peripheral enhancement. She underwent right partial nephrectomy.
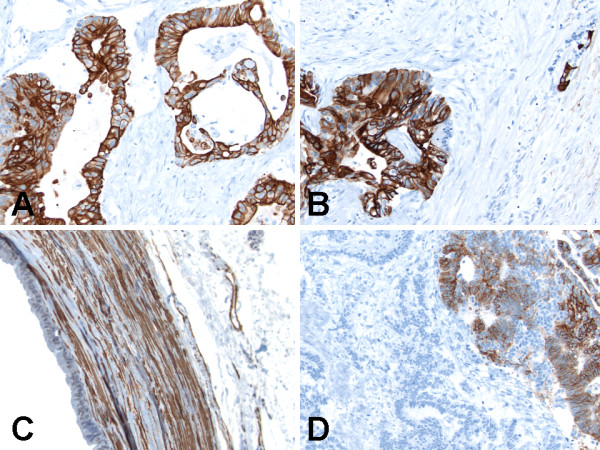
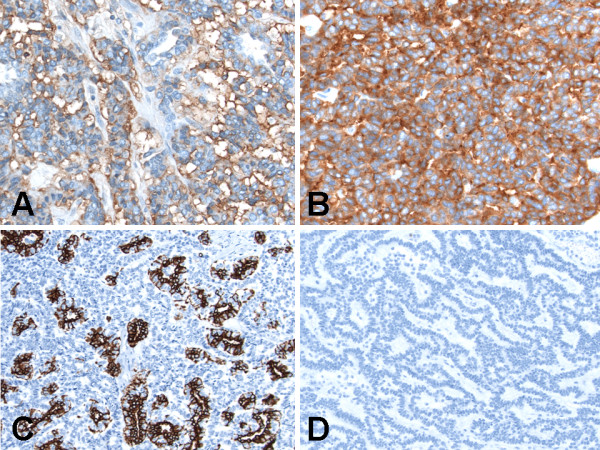
Results: Macroscopically, the encapsulated complex solid and multiloculated cystic tumor with large calcification, focal thickened walls and filled with yellow-tan gelatinous material. Microscopically, the tumor showed coexistent mature cystic teratoma, moderately differentiated adenocarcinoma and carcinoid tumor. Immunohistochemically, alpha-methylacyl-coenzyme A-racemase, calretinin, CD10 and thyroid transcription factor-1 were negative in all the three components of the tumor. The teratomatous cysts lined by ciliated epithelium showed strong staining for cytokeratin 7 and pancytokeratin, and those lined by colonic-like epithelium showed strong staining for CDX2, cytokeratin 20 and pancytokeratin, but both were negative for calretinin. Additionally, the teratomatous cyst wall showed strong staining for smooth muscle actin, and weak staining for carbonic anhydrase IX, CD99, chromogranin and synaptophysin. The adenocarcinoma component was strongly positive for cytokeratin 7 and pancytokeratin, weakly positive for synaptophysin and CD56, and negative for carbonic anhydrase IX, CD99, CDX2, chromogranin, cytokeratin 20 and smooth muscle actin. The carcinoid tumor component was strongly positive for CD56, chromogranin and synaptophysin, weakly positive for pancytokeratin, and negative for carbonic anhydrase IX, CD99, CDX2, cytokeratin 7, cytokeratin 20 and smooth muscle actin. She received no adjuvant therapy and is alive without evidence of disease six months after diagnosis and surgery.
Conclusion: This unique and first case herein presented with synchronous primary carcinoid tumor and primary adenocarcinoma arising within mature cystic teratoma of horseshoe kidney emphasizes the need for thorough sectioning and entire submission for histologic evaluation of mature cystic teratomas, in order to avoid missing multiple additional histogenetically distinct neoplasms.
Figures




References
-
- Resnick ME, Unterberger H, McLoughlin PT. Renal carcinoid producing the carcinoid syndrome. Med Times. 1966;94:895–896. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
