

Soluble fibrillar oligomer levels are elevated in Alzheimer's disease brain and correlate with cognitive dysfunction
- PMID: 19523517
- PMCID: PMC2725199
- DOI: 10.1016/j.nbd.2009.05.024
Soluble fibrillar oligomer levels are elevated in Alzheimer's disease brain and correlate with cognitive dysfunction
Abstract
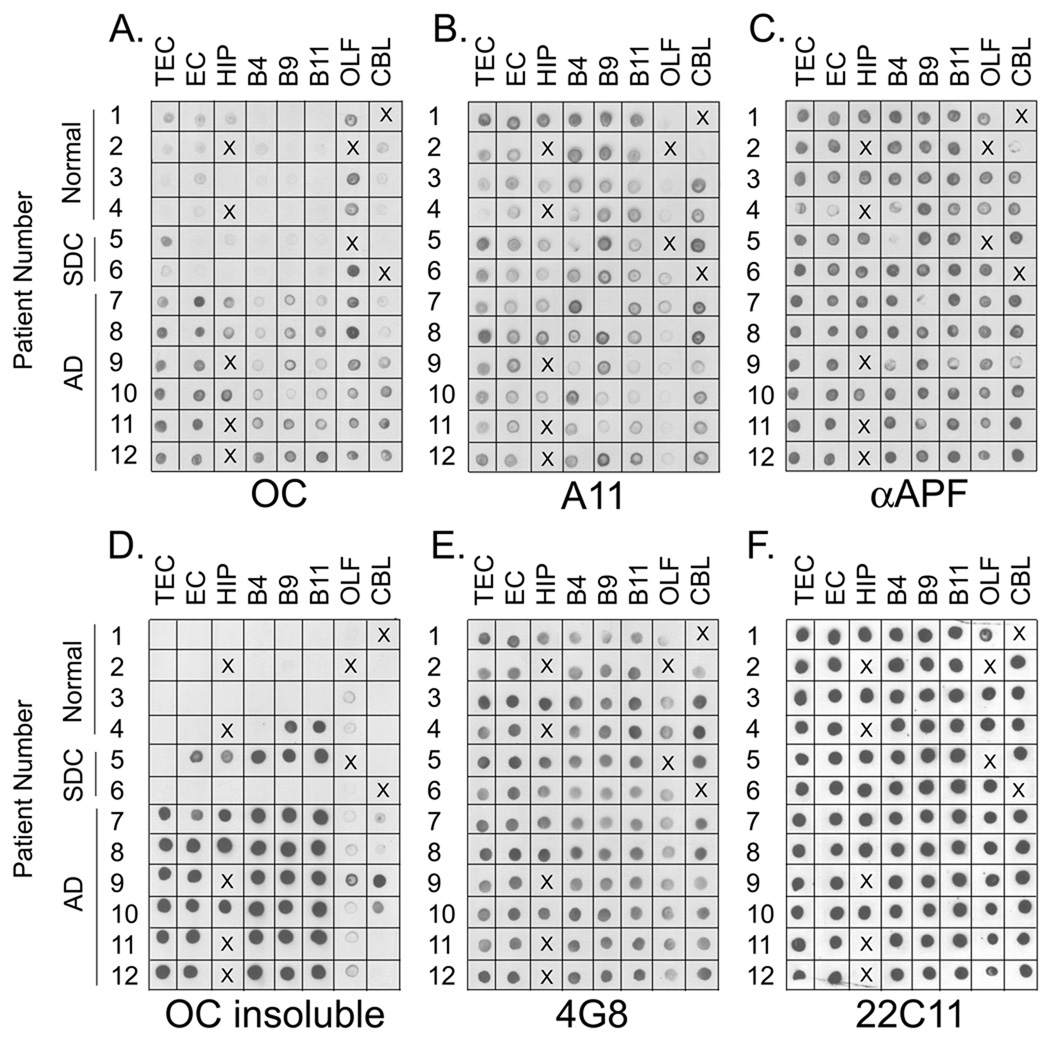
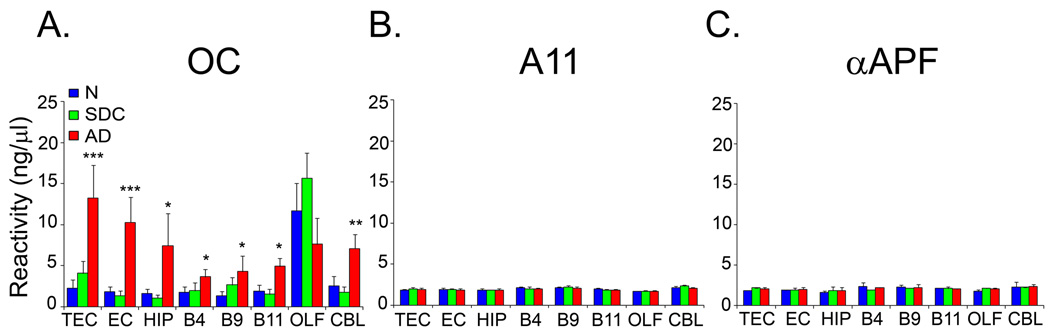
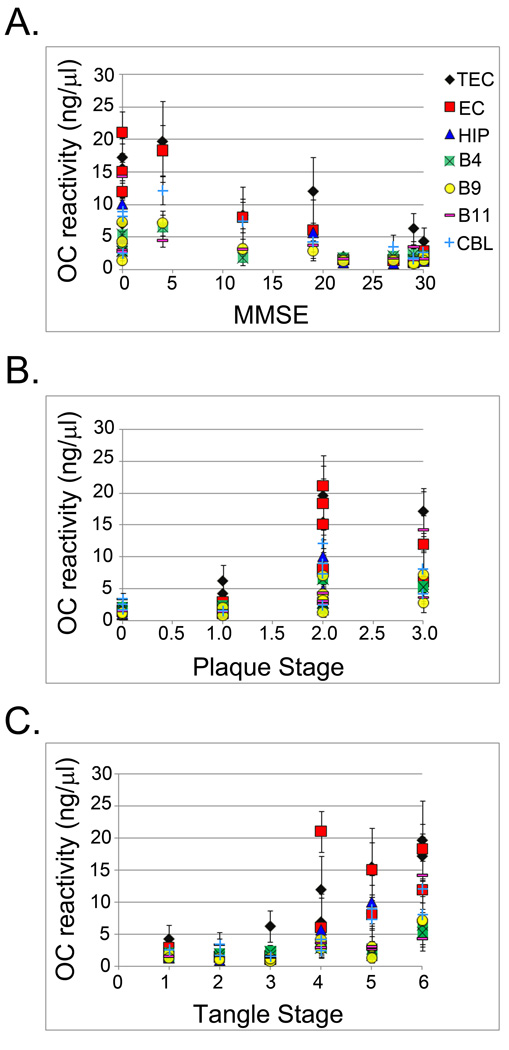
Recent evidence has suggested a role for soluble oligomeric Abeta species in the pathology of Alzheimer's disease (AD). Fibrillar plaque deposits are present in non-demented individuals and levels of soluble Abeta correlate better with cognitive dysfunction in AD and transgenic mouse models. We have previously reported that there are at least two conformationally distinct types of Abeta oligomers: prefibrillar oligomers that are kinetic intermediates in fibril assembly reactions and are specifically recognized by A11 antibody and fibrillar oligomers that may represent fibril seeds or small pieces of fibrils and are recognized by a fibril specific antibody, OC. We have examined the levels of these two types of oligomers in the PBS soluble fraction of brain tissue from control cases, cases with senile degenerative changes (SDC) and AD patients. We found that the levels of soluble fibrillar oligomers detected by OC antibody are significantly elevated in multiple brain regions of AD patients. The elevated fibrillar oligomer levels were found not to be an artifact of tissue homogenization, nor a result of increased Abeta or APP levels. The concentration of fibrillar oligomers in adjacent brain regions of the same patient can vary widely and were not detected in post-mortem cerebrospinal fluid. In contrast, the level of prefibrillar oligomers are variable in both AD and age matched controls, indicating that they are not correlated with cognitive dysfunction and suggesting that they precede dementia in AD. Significant correlations were found between the levels of fibrillar oligomers and cognitive decline (MMSE scores) as well as the neuropathological hallmarks of AD. These results indicate that fibrillar oligomers may play a key role in the pathology of AD and may be a new target for diagnostic and therapeutic development.
Figures
References
-
- Bancher C, Braak H, Fischer P, Jellinger KA. Neuropathological staging of Alzheimer lesions and intellectual status in Alzheime's and Parkinson’s disease patients. Neurosci Lett. 1993;162:179–182. - PubMed
-
- Barghorn S, Nimmrich V, Striebinger A, Krantz C, Keller P, Janson B, Bahr M, Schmidt M, Bitner RS, Harlan J, et al. Globular amyloid beta-peptide oligomer - a homogenous and stable neuropathological protein in Alzheime's disease. J Neurochem. 2005;95:834–847. - PubMed
-
- Bennett DA, Cochran EJ, Saper CB, Leverenz JB, Gilley DW, Wilson RS. Pathological changes in frontal cortex from biopsy to autopsy in Alzheime's disease. Neurobiol Aging. 1993;14:589–596. - PubMed
-
- Blessed G, Tomlinson BE, Roth M. The association between quantitative measures of dementia and of senile change in the cerebral grey matter of elderly subjects. Br J Psychiatry. 1968;114:797–811. - PubMed
-
- Braak H, Braak E. Neuropathological stageing of Alzheimer-related changes. Acta Neuropathol (Berl) 1991;82:239–259. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
