

Isoniazid preventive therapy, HAART and tuberculosis risk in HIV-infected adults in South Africa: a prospective cohort
- PMID: 19525621
- PMCID: PMC3063949
- DOI: 10.1097/QAD.0b013e328327964f
Isoniazid preventive therapy, HAART and tuberculosis risk in HIV-infected adults in South Africa: a prospective cohort
Abstract
Background: The World Health Organization recommends isoniazid preventive therapy (IPT) for preventing tuberculosis in HIV-infected adults, although few countries have instituted this policy. Both IPT and highly active antiretroviral therapy (HAART) used separately result in reductions in tuberculosis risk. There is less information on the combined effect of IPT and HAART. We assessed the effect of IPT, HAART or both IPT and HAART on tuberculosis incidence in HIV-infected adults in South Africa.
Methods: Two clinical cohorts of HIV-infected patients were studied. Primary exposures were receipt of IPT and/or HAART and the primary outcome was incident tuberculosis. Crude incident rates and incident rate ratios were calculated and Cox proportional hazards models investigated associations with tuberculosis risk.
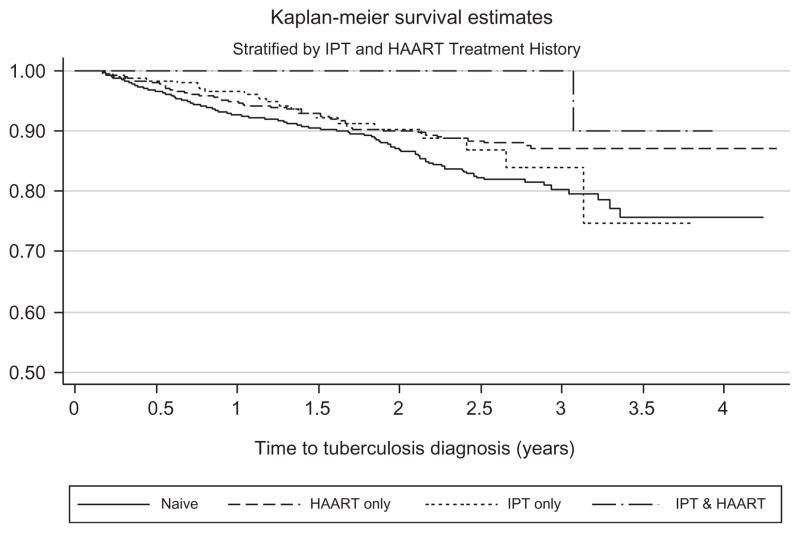
Results: Among 2778 HIV-infected patients followed for 4287 person-years, 267 incident tuberculosis cases were diagnosed [incidence rate ratio (IRR)=6.2/100 person-years; 95% CI 5.5-7.0]. For person-time without IPT or HAART, the IRR was 7.1/100 person-years (95% CI 6.2-8.2); for person-time receiving HAART but without IPT, the IRR was 4.6/100 person-years (95% CI 3.4-6.2); for person-time after IPT but prior to HAART, the IRR was 5.2/100 person-years (95% CI 3.4-7.8); during follow-up in patients treated with HAART after receiving IPT the IRR was 1.1/100 person-years (95% CI 0.02-7.6). Compared to treatment-naive patients, HAART-only patients had a 64% decreased hazard for tuberculosis [adjusted hazard ratio (aHR)=0.36; 95% CI 0.25-0.51], and patients receiving HAART after IPT had a 89% reduced hazard (aHR=0.11; 95% CI 0.02-0.78).
Conclusion: Tuberculosis risk is significantly reduced by IPT in HAART-treated adults in a high-incidence operational setting in South Africa. IPT is an inexpensive and cost-effective strategy and our data strengthen calls for the implementation of IPT in conjunction with the roll-out of HAART.
Figures
Comment in
-
Are the effects of isoniazid preventive therapy and highly active antiretroviral therapy additive in preventing HIV-associated tuberculosis?AIDS. 2009 Jul 17;23(11):1444-6. doi: 10.1097/QAD.0b013e32832d53e7. AIDS. 2009. PMID: 19564724 Free PMC article. No abstract available.
References
-
- Comstock GW, Ferebee SH, Hammes LM. A controlled trial of community-wide isoniazid prophylaxis in Alaska. Am Rev Respir Dis. 1967;95:935–943. - PubMed
-
- Ferebee SH. Controlled chemoprophylaxis trials in tuberculosis. A general review. Bibl Tuberc. 1970;26:28–106. - PubMed
-
- Ferebee SH. Long-term effects of isoniazid prophylaxis. Bull Int Union Tuberc. 1968;41:161–166. - PubMed
-
- Pape JW, Jean SS, Ho JL, Hafner A, Johnson WD., Jr Effect of isoniazid prophylaxis on incidence of active tuberculosis and progression of HIV infection. Lancet. 1993;342:268–272. - PubMed
-
- Mwinga A, Hosp M, Godfrey-Faussett P, Quigley M, Mwaba P, Mugala BN, et al. Twice weekly tuberculosis preventive therapy in HIV infection in Zambia. AIDS. 1998;12:2447–2457. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
