

Similar progression of diabetic retinopathy with insulin glargine and neutral protamine Hagedorn (NPH) insulin in patients with type 2 diabetes: a long-term, randomised, open-label study
- PMID: 19526210
- PMCID: PMC2723680
- DOI: 10.1007/s00125-009-1415-7
Similar progression of diabetic retinopathy with insulin glargine and neutral protamine Hagedorn (NPH) insulin in patients with type 2 diabetes: a long-term, randomised, open-label study
Abstract
Aims/hypothesis: This long-term study was designed to further characterise the retinal safety profile of insulin glargine and human neutral protamine Hagedorn (NPH) insulin in patients with type 2 diabetes mellitus.
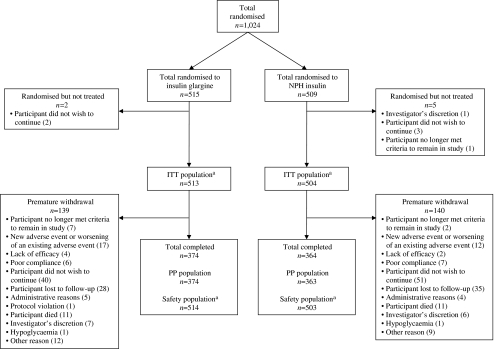
Methods: An open-label, 5 year, randomised (1:1), multicentre, stratified, parallel-group study conducted in the USA and Canada enrolled individuals with type 2 diabetes and either no or non-proliferative retinopathy (less than severe; Early Treatment Diabetic Retinopathy Study [ETDRS] level less than 53 in both eyes) who were treated with oral hypoglycaemic agents (OHAs) alone, insulin alone or OHAs with insulin for >/=3 months prior to study entry and a baseline HbA(1c) level of 6.0-12.0%. Patients were randomised by the investigator according to the centralised interactive voice response system to receive twice-daily NPH insulin (n = 509) or once-daily basal insulin glargine (n = 515). The investigator was not blinded to the treatment group to which each participant had been assigned. The main objective of this study was to compare the progression of diabetic retinopathy between treatment groups by analysing the percentage of patients with three or more step progression in the ETDRS retinopathy patient-level severity scale after treatment with either basal insulin. Masked, centralised grading of seven-field stereoscopic fundus photographs was used.
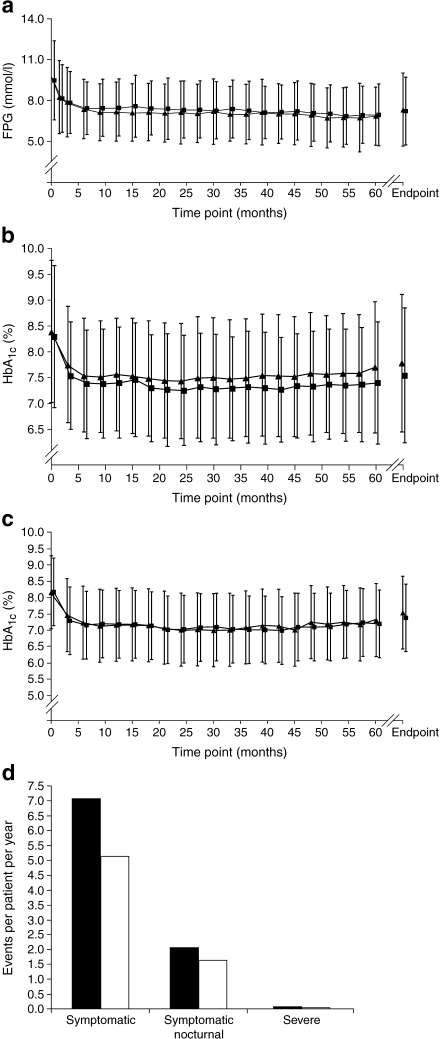
Results: Similarly sustained glycaemic control was observed in both the insulin glargine and NPH insulin treatment groups. Despite a slightly greater severity of diabetic retinopathy for the insulin glargine group at baseline, three or more step progression in ETDRS score from baseline to end-of-study was similar between treatment groups (14.2% [53/374] of insulin glargine-treated patients vs 15.7% [57/363] of NPH-treated patients); the difference in the incidence of progression was -1.98% (95% CI -7.02, 3.06%). Other measures of retinopathy-the development of proliferative diabetic retinopathy and progression to clinically significant macular oedema-occurred to a similar degree in both treatment groups. No other safety issues, such as unexpected adverse events for either insulin emerged during the 5 year study. However, NPH insulin treatment was associated with a higher incidence of severe hypoglycaemia compared with insulin glargine.
Conclusions/interpretation: This study shows no evidence of a greater risk of the development or progression of diabetic retinopathy with insulin glargine vs NPH insulin treatment in patients with type 2 diabetes mellitus.
Trial registration: ClinicalTrials.gov NCT00174824
Funding: This study was sponsored by sanofi-aventis.
Figures

Comment in
-
The longest ever randomised controlled trial of insulin glargine: study design and HbA(1c) findings.Diabetologia. 2009 Oct;52(10):2234-5; author reply 2236-9. doi: 10.1007/s00125-009-1477-6. Epub 2009 Aug 7. Diabetologia. 2009. PMID: 19662377 No abstract available.
-
Diabetic retinopathy and insulin glargine.Diabetologia. 2009 Oct;52(10):2233; author reply 2236-9. doi: 10.1007/s00125-009-1488-3. Epub 2009 Aug 14. Diabetologia. 2009. PMID: 19680626 No abstract available.
References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1038/ki.1995.236', 'is_inner': False, 'url': 'https://doi.org/10.1038/ki.1995.236'}, {'type': 'PubMed', 'value': '7643540', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/7643540/'}]}
- Diabetes Control and Complications Trial Research Group (1995) Effect of intensive therapy on the development and progression of diabetic nephropathy in the Diabetes Control and Complications Trial. The Diabetes Control and Complications (DCCT) Research Group. Kidney Int 47:1703–1720 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1007/s001250051594', 'is_inner': False, 'url': 'https://doi.org/10.1007/s001250051594'}, {'type': 'PubMed', 'value': '11270671', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/11270671/'}]}
- Stratton IM, Kohner EM, Aldington SJ et al (2001) UKPDS 50: risk factors for incidence and progression of retinopathy in type II diabetes over 6 years from diagnosis. Diabetologia 44:156–163 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1056/NEJMoa0806470', 'is_inner': False, 'url': 'https://doi.org/10.1056/nejmoa0806470'}, {'type': 'PubMed', 'value': '18784090', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/18784090/'}]}
- Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA (2008) 10-Year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med 359:1577–1589 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1016/S0140-6736(98)07019-6', 'is_inner': False, 'url': 'https://doi.org/10.1016/s0140-6736(98)07019-6'}, {'type': 'PubMed', 'value': '9742976', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/9742976/'}]}
- UK Prospective Diabetes Study (UKPDS) Group (1998) Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 352:837–853 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1056/NEJM199309303291401', 'is_inner': False, 'url': 'https://doi.org/10.1056/nejm199309303291401'}, {'type': 'PubMed', 'value': '8366922', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/8366922/'}]}
- Diabetes Control and Complications Trial Research Group (1993) The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 329:977–986 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
