

Posterior-only multilevel modified vertebral column resection for extremely severe Pott's kyphotic deformity
- PMID: 19526375
- PMCID: PMC2899371
- DOI: 10.1007/s00586-009-1067-9
Posterior-only multilevel modified vertebral column resection for extremely severe Pott's kyphotic deformity
Abstract
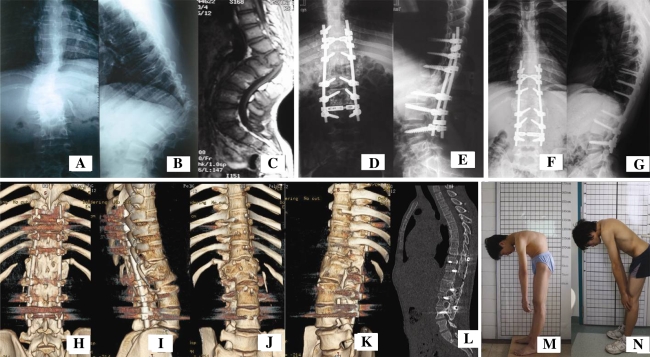
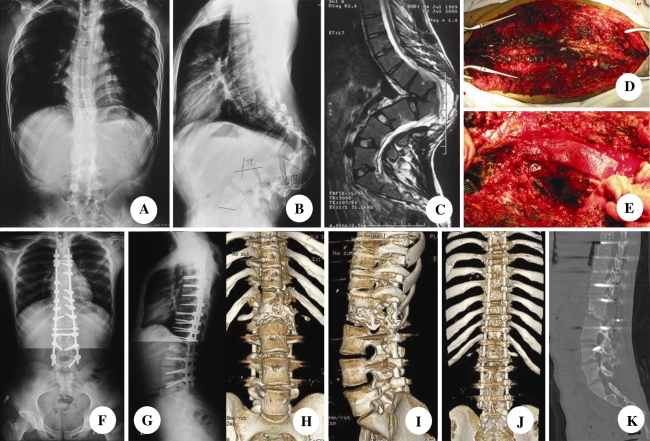
Extremely severe Pott's kyphotic deformity cannot be completely corrected by conventional techniques, including vertebral body resection, Smith-Peterson, pedicle subtraction osteotomy or even vertebral column resection (VCR). The authors developed a new technique combining transpedicular eggshell osteotomies and VCR as multilevel modified vertebral column resection (MVCR) through a single posterior approach for surgical treatment of Pott's kyphosis with Konstam's angle beyond 90 degrees. A total of 9 patients (6 males, 3 females) in our institution with severe Pott's kyphosis who underwent single-stage posterior-only multilevel MVCR were retrospectively reviewed. The candidates for multilevel MVCR were those with a sharp, angular kyphosis in the lower thoracic or upper lumbar spine with a Konstam's angle beyond 90 degrees. The follow-up averaged 30.6 months (ranging from 21 to 50 months). Fusion status was evaluated at each follow-up by CT three-dimensional reconstruction images. An average of 2.5 vertebrae was removed in each case (ranging from 2 to 4 vertebrae). A mean of 7 vertebrae were fused (ranging from 6 to 11 vertebrae). The mean duration of surgery was 285 min (ranging from 246 to 400 min), the average intraoperative blood loss was 2,933 ml (ranging from 2,000 to 6,000 ml). The mean preoperative kyphus was 100.3 degrees (ranging from 90 degrees to 132 degrees ). The mean kyphosis in the immediate postoperative period was 15.9 degrees (ranging from 4 degrees to 30 degrees) with an average postoperative kyphos correction of 84.4 degrees (ranging from 63 degrees to 126 degrees). Fusion of the resection site was confirmed on radiographs in all patients at the minimum 12 months follow-up. No pseudoarthrosis was found. No loosening or breakage of pedicle screws occurred. A single-stage posterior-only multilevel MVCR is an effective way to correct extremely severe Pott's kyphosis with Konstam's angle beyond 90 degrees.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
