

Switching to second-line antiretroviral therapy in resource-limited settings: comparison of programmes with and without viral load monitoring
- PMID: 19531928
- PMCID: PMC2956749
- DOI: 10.1097/QAD.0b013e32832e05b2
Switching to second-line antiretroviral therapy in resource-limited settings: comparison of programmes with and without viral load monitoring
Abstract
Background: In high-income countries, viral load is routinely measured to detect failure of antiretroviral therapy (ART) and guide switching to second-line ART. Viral load monitoring is not generally available in resource-limited settings. We examined switching from nonnucleoside reverse transcriptase inhibitor (NNRTI)-based first-line regimens to protease inhibitor-based regimens in Africa, South America and Asia.
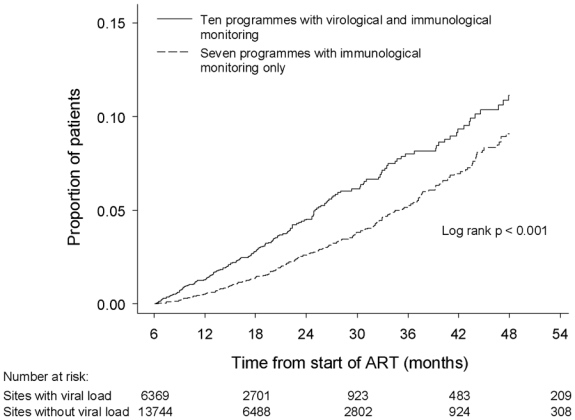
Design and methods: Multicohort study of 17 ART programmes. All sites monitored CD4 cell count and had access to second-line ART and 10 sites monitored viral load. We compared times to switching, CD4 cell counts at switching and obtained adjusted hazard ratios for switching (aHRs) with 95% confidence intervals (CIs) from random-effects Weibull models.
Results: A total of 20 113 patients, including 6369 (31.7%) patients from 10 programmes with access to viral load monitoring, were analysed; 576 patients (2.9%) switched. Low CD4 cell counts at ART initiation were associated with switching in all programmes. Median time to switching was 16.3 months [interquartile range (IQR) 10.1-26.6] in programmes with viral load monitoring and 21.8 months (IQR 14.0-21.8) in programmes without viral load monitoring (P < 0.001). Median CD4 cell counts at switching were 161 cells/microl (IQR 77-265) in programmes with viral load monitoring and 102 cells/microl (44-181) in programmes without viral load monitoring (P < 0.001). Switching was more common in programmes with viral load monitoring during months 7-18 after starting ART (aHR 1.38; 95% CI 0.97-1.98), similar during months 19-30 (aHR 0.97; 95% CI 0.58-1.60) and less common during months 31-42 (aHR 0.29; 95% CI 0.11-0.79).
Conclusion: In resource-limited settings, switching to second-line regimens tends to occur earlier and at higher CD4 cell counts in ART programmes with viral load monitoring compared with programmes without viral load monitoring.
2009 Wolters Kluwer Health | Lippincott Williams & Wilkins
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Palella FJ, Delaney KM, Moorman AC, Loveless MO, Fuhrer J, Satten GA, et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. N Engl J Med. 1998;338:853–860. - PubMed
-
- Mocroft A, Vella S, Benfield TL, Chiesi A, Miller VT, Gargalianos P, et al. Changing patterns of mortality across Europe in patients infected with HIV-1. Lancet. 1998;352:1725–1730. - PubMed
-
- World Health Organization. World Health Organization. Progress report 2008. Geneva: WHO; 2008. [(accessed February 2009)]. Towards universal access. Scaling up priority HIV/AIDS interventions in the health sector. Available at http://www.who.int/hiv/mediacenter/universal_access_progres_report_en.pdf.
-
- Hammer SM, Eron JJ, Jr, Reiss P, Schooley RT, Thompson MA, Walmsley S, et al. Antiretroviral treatment of adult HIV infection: 2008 recommendations of the International AIDS Society-USA panel. JAMA. 2008;300(5):555–570. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
