

Primary cardiac diffuse large B cell lymphoma presenting with superior vena cava syndrome
- PMID: 19536397
- PMCID: PMC2722499
- DOI: 10.1016/s0828-282x(09)70110-2
Primary cardiac diffuse large B cell lymphoma presenting with superior vena cava syndrome
Abstract
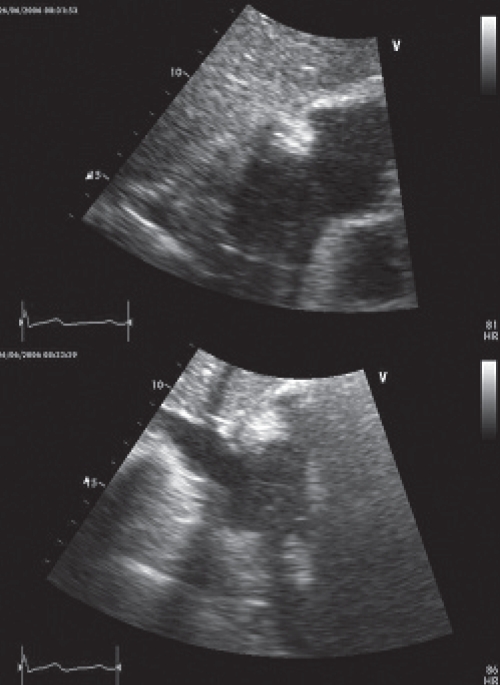
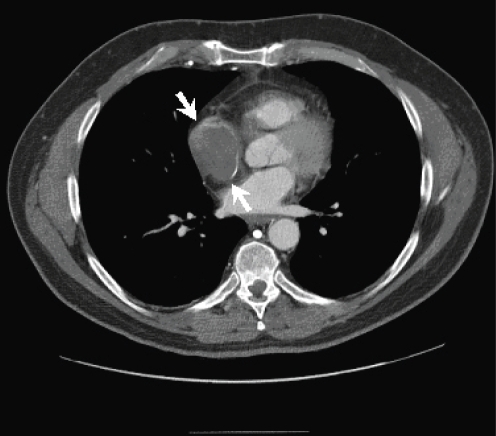
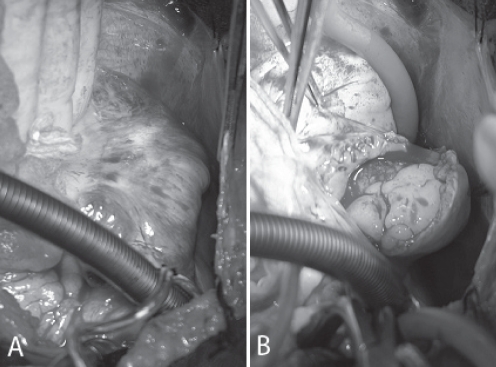
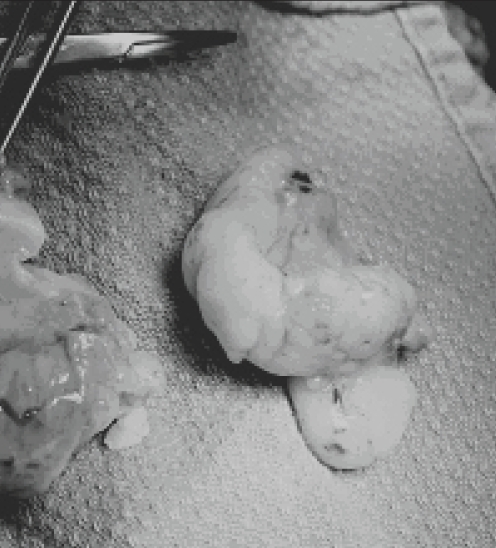
Primary cardiac lymphomas are rare extranodal lymphomas that should be distinguished from secondary cardiac involvement by disseminated non-Hodgkin's lymphoma. Cardiac lymphomas often mimic other cardiac neoplasms, including myxomas and angiosarcomas, and often require multimodality cardiac imaging, in combination with endomyocardial biopsy, excisional biopsy or pericardial fluid cytology, to establish a definitive diagnosis. A 60-year-old immunocompetent man who presented with superior vena cava syndrome secondary to a right atrial, primary cardiac diffuse large B cell lymphoma (non-Hodgkin's lymphoma) is described in the present article. The patient had no clinical evidence of disseminated lymphoma and was successfully treated with prompt surgical excision of his atrial mass, followed by anthracycline-based chemotherapy. The patient required multi-modality cardiac imaging to accurately identify and plan surgical excision of his cardiac lymphoma. The therapeutic management and clinical and radio-logical features of primary cardiac lymphoma are reviewed.
Les lymphomes cardiaques primaires sont des lymphomes extranodaux rares qu’il faudrait distinguer d’une atteinte cardiaque secondaire par lymphome non hodgkinien disséminé. Les lymphomes cardiaques imitent souvent d’autres néoplasmes cardiaques, y compris les myxomes et les angiosarcomes, et exigent souvent une imagerie cardiaque multimode, conjointement avec une biopsie endomyocardique, une biopsie-exérèse ou une cytologie du liquide péricardique, afin de poser un diagnostic définitif. Un homme immunocompétent de 60 ans qui a consulté en raison d’un syndrome de compression de la veine cave supérieure secondaire à un lymphome cardiaque primaire diffus à grandes cellules bêta (lymphome non hodgkinien) est décrit dans le présent article. Le patient ne présentait aucune constatation clinique de lymphome disséminé et a reçu un traitement concluant par excision chirurgicale rapide de la masse auriculaire, suivi d’une chimiothérapie à l’anthracycline. Il a dû subir une imagerie cardiaque multimode pour repérer avec précision et planifier l’excision chirurgicale du lymphome cardiaque. L’auteur examine la prise en charge thérapeutique et les caractéristiques cliniques et radiologiques du lymphome cardiaque primaire.
Figures

References
-
- Burke A, Virmani R. Atlas of Tumor Pathology (Third series, fascicle 16): Tumors of the Heart and Great Vessels. Washington: Armed Forces Institute of Pathology; 1996. pp. 171–9.
-
- Ceresoli GL, Ferreri AJM, Bucci E, Ripa C, Ponzoni M, Villa E. Primary cardiac lymphoma in immunocompetent patients: Diagnostic and therapeutic management. Cancer. 1997;80:1497–506. - PubMed
-
- Nascimento AF, Winters GL, Pinkus GS. Primary cardiac lymphoma: Clinical, histologic, immunophenotypic, and genotypic features of 5 cases of a rare disorder. Am J Surg Pathol. 2007;31:1344–50. - PubMed
-
- Schell AJ, Xu Y, Baetz T, et al. Primary cardiac lymphoma: Molecular cytogenetic characterization of a rare entity. Cardiovasc Pathol. 2009;18:92–9. - PubMed
-
- Rolla G, Galligaris-Cappio F, Burke AP. Cardiac lymphomas. In: Travis WD, Brambilla E, Muller-Hermelink HK, Harris CC, editors. World Health Organization Classification of Tumours Pathology and Genetics of Tumours of the Lung, Pleura, Thymus and Heart. 1st edn. Lyon: IARC Press; 2004. pp. 282–3.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
