

Can local application of Tranexamic acid reduce post-coronary bypass surgery blood loss? A randomized controlled trial
- PMID: 19538741
- PMCID: PMC2706826
- DOI: 10.1186/1749-8090-4-25
Can local application of Tranexamic acid reduce post-coronary bypass surgery blood loss? A randomized controlled trial
Abstract
Background: Diffuse microvascular bleeding remains a common problem after cardiac procedures. Systemic use of antifibrinolytic reduces the postoperative blood loss. The purpose of this study was to examine the effectiveness of local application of tranexamic acid to reduce blood loss after coronary artery bypass grafting (CABG).
Methods: Thirty eight patients scheduled for primary isolated coronary artery bypass grafting were included in this double blind, prospective, randomized, placebo controlled study. Tranexamic acid (TA) group (19 patients) received 1 gram of TA diluted in 100 ml normal saline. Placebo group (19 patients) received 100 ml of normal saline only. The solution was purred in the pericardial and mediastinal cavities.
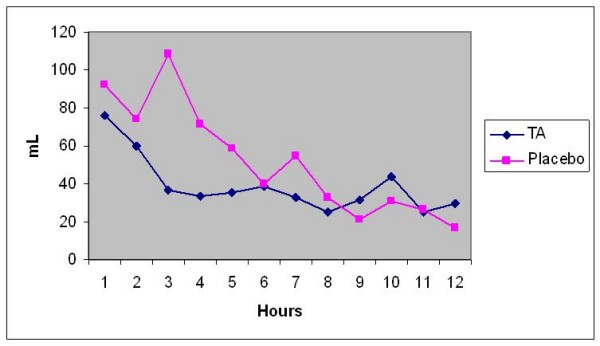
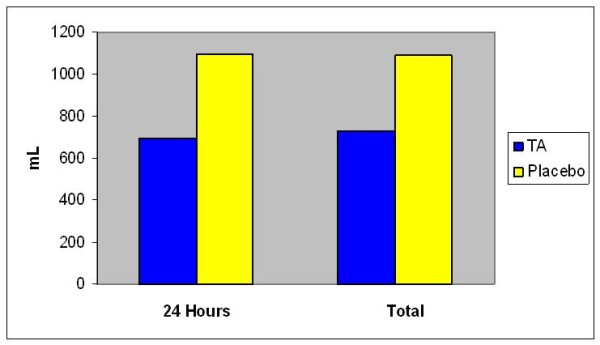
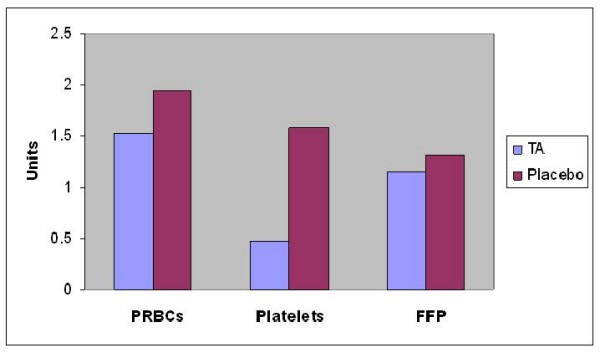
Results: Both groups were comparable in their baseline demographic and surgical characteristics. During the first 24 hours post-operatively, cumulative blood loss was significantly less in TA group (median of 626 ml) compared to Placebo group (median of 1040 ml) (P = 0.04). There was no significant difference in the post-op Packed RBCs transfusion between both groups (median of one unit in each) (P = 0.82). Significant less platelets transfusion required in TA group (median zero unit) than in placebo group (median 2 units) (P = 0.03). Apart from re-exploration for excessive surgical bleeding in one patient in TA group, no difference was found in morbidity or mortality between both groups.
Conclusion: Topical application of tranexamic acid in patients undergoing primary coronary artery bypass grafting led to a significant reduction in postoperative blood loss without adding extra risk to the patient.
Figures
References
-
- Harker LA, Malpass TW, Branson HE, Hessel EA, II, Slichter SJ. Mechanism of abnormal bleeding in patients undergoing cardiopulmonary bypass: acquired transient platelet dysfunction associated with selective alpha-granule release. Blood. 1980;56:824–34. - PubMed
-
- Depotis GJ, Santoro SA, Spitznagel E, Kater KM, Cox JL, Barnes P. Prospective evaluation and clinical utility of on-site monitoring of coagulation in patients undergoing cardiac operation. J Thorac Cardiovasc Surg . 1994;107:271–279. - PubMed
-
- Lemmer JH, Jr, Stanford W, Bonney SL, Breen JF, Chomka EV, Elderge WJ. Aprotonin for coronary bypass operations: efficacy, safety, and influence on early saphenous graft patency-a multicenter, randomized, double blind, placebo-controlled study. J Thorac Cardiovasc Surg. 1994;107:543–53. - PubMed
-
- Daily PO, Lamphere JA, Dembitsky WP, Adamson RM, Dans NF. Effect of prophylactic epsilon-aminocaproic acid on blood loss and transfusion requitments in patients undergoing first-time coronary artery bypass grafting: a randomized, prospective, double-blind study. J Thorac Cardiovasc Surg. 1994;108:99–105. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
