

Enhanced central pain processing of fibromyalgia patients is maintained by muscle afferent input: a randomized, double-blind, placebo-controlled study
- PMID: 19540671
- PMCID: PMC2751583
- DOI: 10.1016/j.pain.2009.05.020
Enhanced central pain processing of fibromyalgia patients is maintained by muscle afferent input: a randomized, double-blind, placebo-controlled study
Abstract
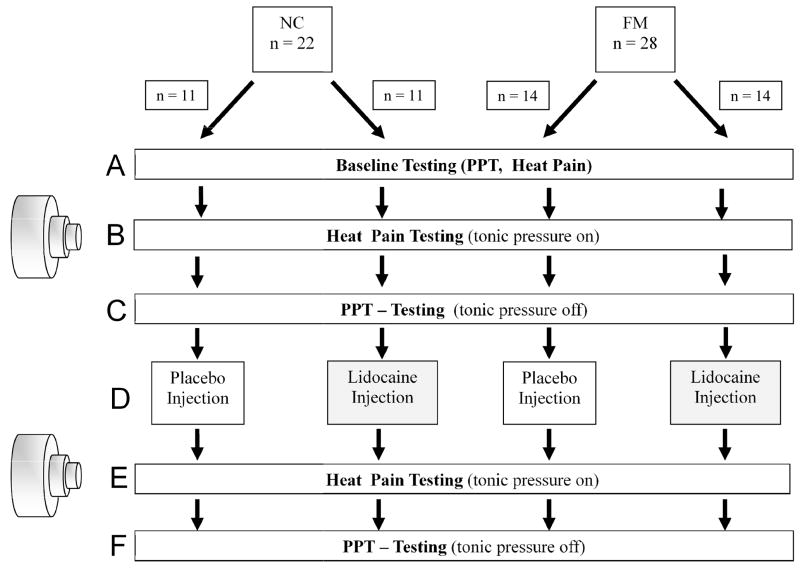
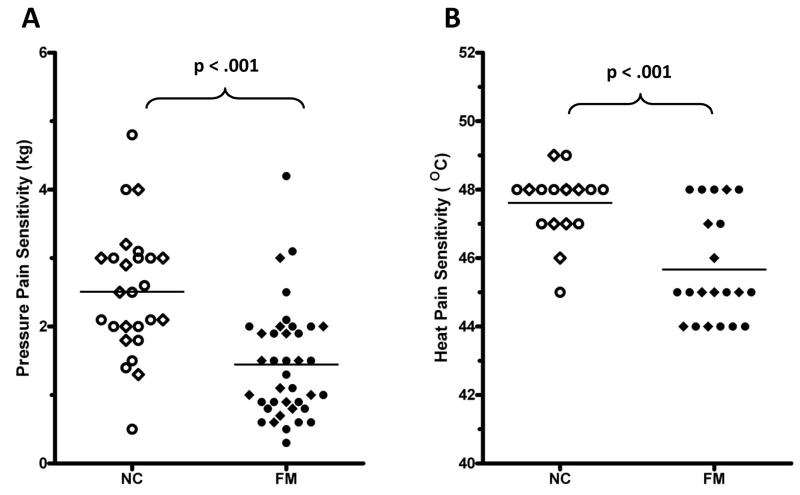
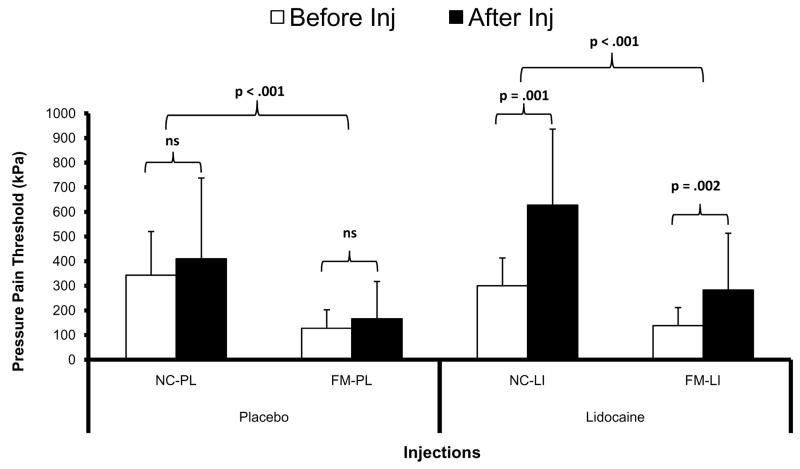
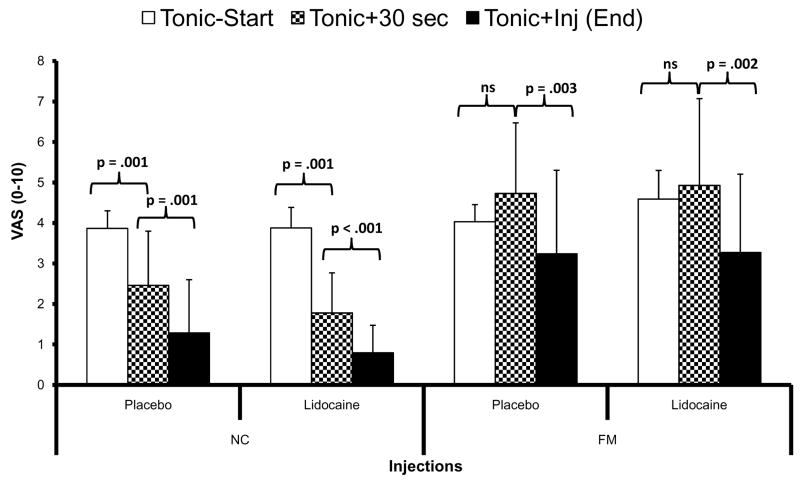
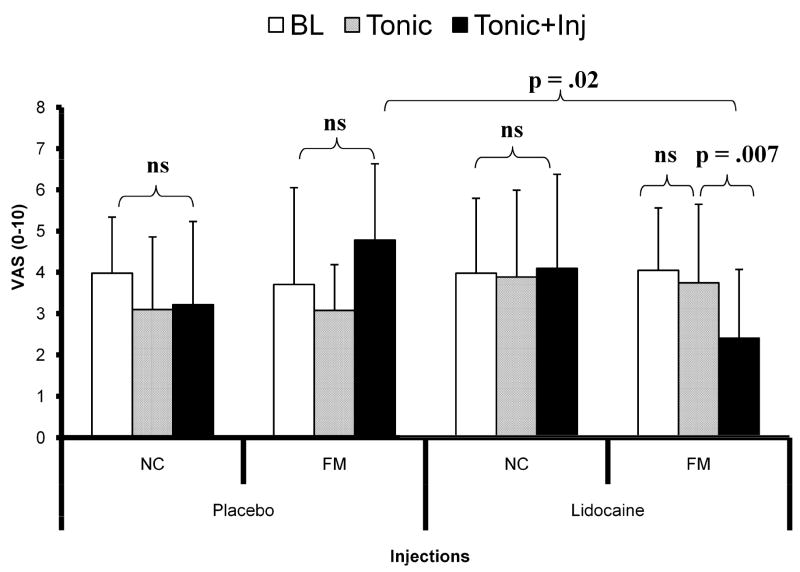
Fibromyalgia (FM) syndrome is characterized by pain and widespread hyperalgesia to mechanical, thermal, and electrical stimuli. Despite convincing evidence for central sensitization of nociceptive pain pathways, the role of peripheral tissue impulse input in the initiation and maintenance of FM is unclear. Therefore this randomized, double-blind, placebo-controlled trial of 22 female normal controls (NCs) and 28 female FM subjects tested the effects of trapezius muscle (TrapM) tender point injections with 1% lidocaine on local pain thresholds as well as on remote heat hyperalgesia at the forearm. Prior to muscle injections shoulder pain was standardized by tonic mechanical muscle stimulation, resulting in local pain ratings of 4.0+/-0.5 VAS units. Tonic muscle stimulation was interrupted for the TrapM injections but was continued afterwards at the same level. NC as well as FM subjects experienced significant increases of TrapM pressure pain thresholds from lidocaine injections but not from placebo injections (p<0.001). Additionally, heat hyperalgesia of FM participants was significantly reduced at areas remote from the injection site (forearm) by lidocaine but not by placebo (p=0.02). Neither lidocaine nor saline injections significantly affected clinical FM pain ratings, a result most likely due to the very low dose of lidocaine (50mg) used in this trial.
Conclusion: Lidocaine injections increased local pain thresholds and decreased remote secondary heat hyperalgesia in FM patients, emphasizing the important role of peripheral impulse input in maintaining central sensitization in this chronic pain syndrome; similar to other persistent pain conditions such as irritable bowel syndrome and complex regional pain syndrome.
Conflict of interest statement
The authors have no financial or other relationships to report that might result in a conflict of interest.
Figures
References
-
- Arendt-Nielsen L, Graven-Nielsen T. Muscle pain: sensory implications and interaction with motor control. Clin J Pain. 2008;24:291–8. - PubMed
-
- Arendt-Nielsen L, Svensson P. Referred muscle pain: basic and clinical findings. Clin J Pain. 2001;17:11–9. - PubMed
-
- Bajaj P, Bajaj P, Madsen H, Moller M, Arendt-Nielsen L. Antenatal women with or without pelvic pain can be characterized by generalized or segmental hypoalgesia in late pregnancy. J Pain. 2002;3:451–60. - PubMed
-
- Bartels EM, Danneskiold-Samsoe B. Histological abnormalities in muscle from patients with certain types of fibrositis. Lancet. 1986;1:755–7. - PubMed
-
- Bengtsson A. The muscle in fibromyalgia. Rheumatology. 2002;41:721–4. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
