

Renal impairment after liver transplantation - a pilot trial of calcineurin inhibitor-free vs. calcineurin inhibitor sparing immunosuppression in patients with mildly impaired renal function after liver transplantation
- PMID: 19541578
- PMCID: PMC3351980
- DOI: 10.1186/2047-783x-14-5-210
Renal impairment after liver transplantation - a pilot trial of calcineurin inhibitor-free vs. calcineurin inhibitor sparing immunosuppression in patients with mildly impaired renal function after liver transplantation
Abstract
Objectives: Chronic kidney disease is frequent in patients after orthotopic liver transplantation (OLT) and has impact on survival. Patients receiving calcineurin inhibitors (CNI) are at increased risk to develop impaired renal function. Early CNI reduction and concomitant use of mycophenolat mofetil (MMF) has been shown to improve renal function.
Methods: The aim of this trial was to compare dose-reduced CNI/MMF versus CNI-free MMF/prednisone-based treatment in stable patients after OLT with respect to glomerular filtration rate (GFR). 21 patients (GFR 44.9 ' 9.9 mL/min/1.73m2 measured by 99m-Tc-DTPA-clearance, serum creatinine (SCr) 1.5 ' 0.42 mg/dL) were randomized either to exchange CNI for 10 mg prednisone (group 1; n = 8) or to receive CNI at 25% of the initial dose (group 2; n = 13) each in combination with 1000 mg MMF b.i.d.
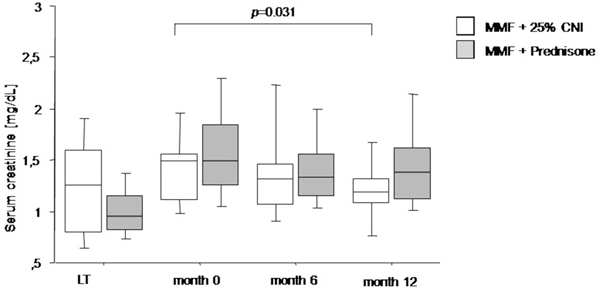
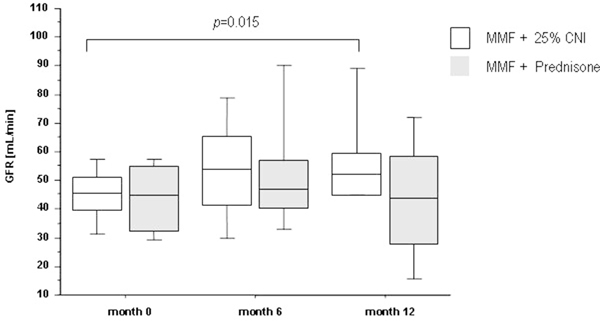
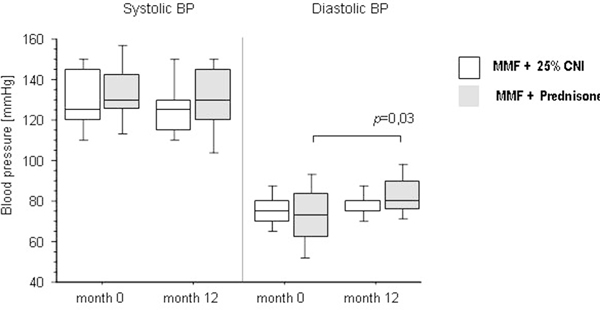
Results: At month 12 mean SCr (-0.3 ' 0.4 mg/dL, p = 0.031) and GFR improved (8.6 ' 13.1 mL/min/ 1.73m superset2, p = 0.015) in group 2 but remained unchanged in group 1. Main side effects were gastroinstestinal symptoms (14.3%) and infections (4.8%). Two biopsy proven, steroid-responsive rejections occurred. In group 1 mean diastolic blood pressure (BP) increased by 11 ' 22 mmHg (p = 0.03).
Conclusions: Reduced dose CNI in combination with MMF but not CNI-free-immunosuppression leads to improvement of GFR in patients with moderately elevated SCr levels after OLT. Addition of steroids resulted in increased diastolic blood pressure presumably counterbalancing the benefits of CNI withdrawal on renal function.
Figures
References
-
- Gonwa TA, Mai ML, Melton LB, Hays SR, Goldstein RM, Levy MF, Klintmalm GB. End-stage renal disease (ESRD) after orthotopic liver transplantation (OLTX) using calcineurin-based immunotherapy: risk of development and treatment. Transplantation. 2001;72(12):1934–1939. doi: 10.1097/00007890-200112270-00012. - DOI - PubMed
-
- Schlitt HJ, Barkmann A, Boker KH, Schmidt HH, Emmanouilidis N, Rosenau J, Bahr MJ, Tusch G, Manns MP, Nashan B, Klempnauer J. Replacement of calcineurin inhibitors with mycophenolate mofetil in liver-transplant patients with renal dysfunction: a randomised controlled study. Lancet. 2001;357(9256):587–591. doi: 10.1016/S0140-6736(00)04055-1. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
