

Natural history, clinical pattern, and surgical considerations of pneumatosis intestinalis
- PMID: 19541582
- PMCID: PMC3352014
- DOI: 10.1186/2047-783x-14-6-231
Natural history, clinical pattern, and surgical considerations of pneumatosis intestinalis
Abstract
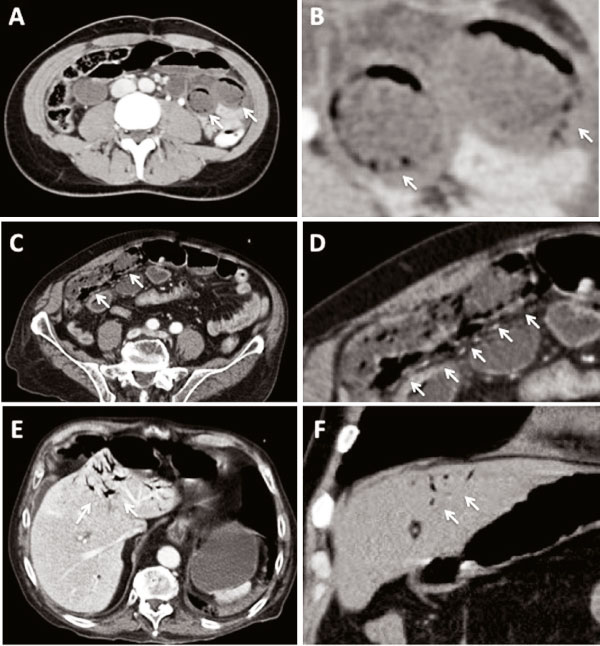
Objective: Pneumatosis intestinalis has been increasingly detected in recent years with the more frequent use of computed tomography for abdominal imaging of the intestine. The underlying causes of the gas found during radiographic studies of the bowel wall can vary widely and different hypotheses regarding its pathophysiology have been postulated. Pneumatosis intestinalis often represents a benign condition and should not be considered an argument for surgery. However, it can also require life-threatening surgery in some cases, and this can be a difficult decision in some patients.
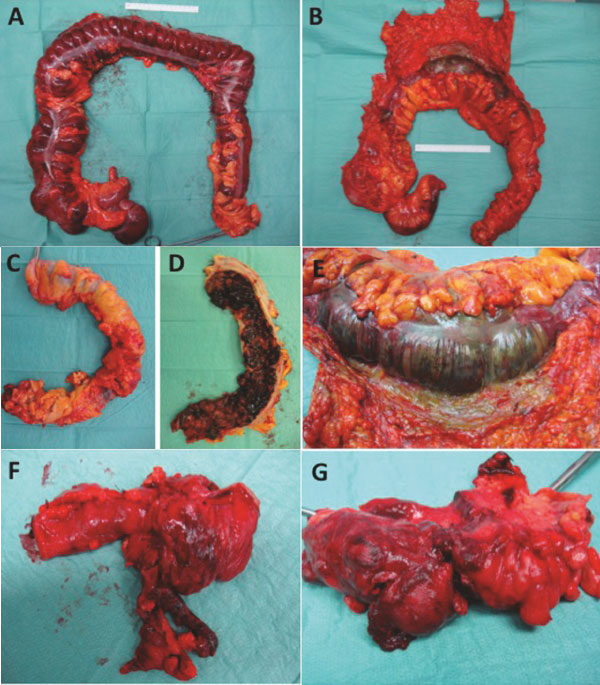
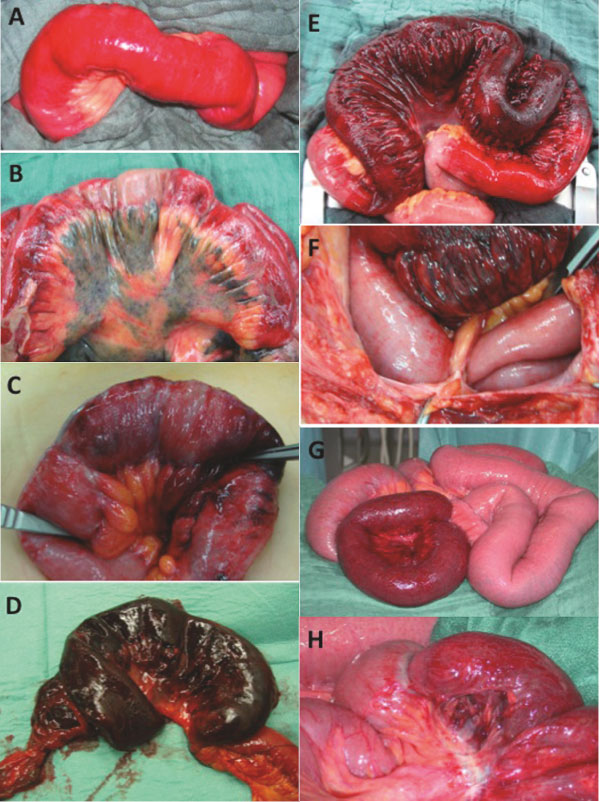
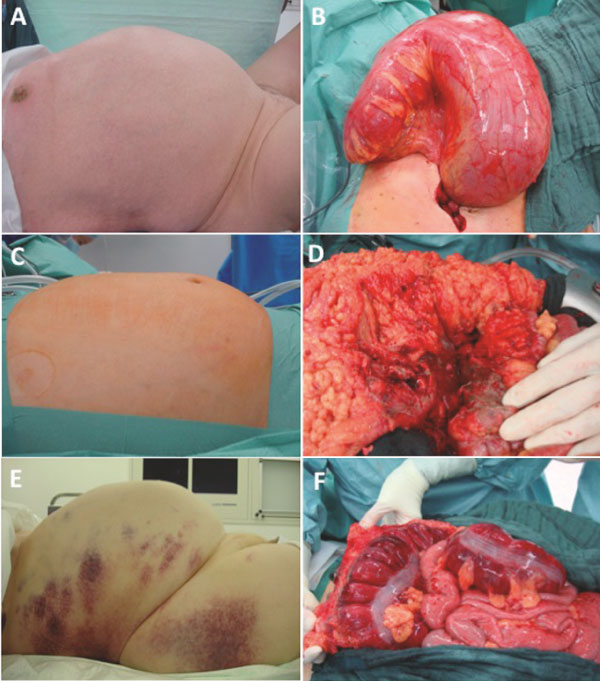
Methods: The spectrum of pneumatosis intestinalis is discussed here based on various computed tomographic and surgical findings in patients who presented at our University Medical Centre in 2003-2008. We have also systematically reviewed the literature to establish the current understanding of its aetiology and pathophysiology, and the possible clinical conditions associated with pneumatosis intestinalis and their management.
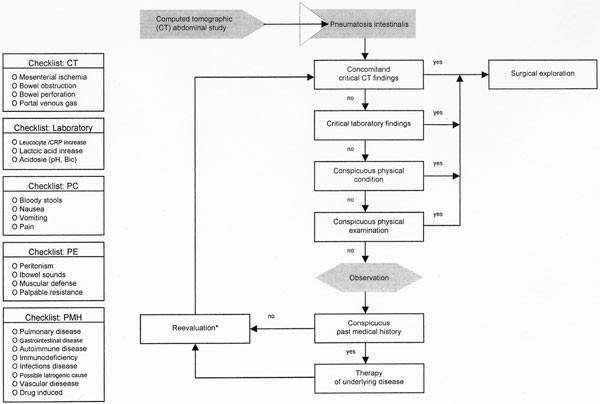
Results: Pneumatosis intestinalis is a primary radiographic finding. After its diagnosis, its specific pathogenesis should be ascertained because the appropriate therapy is related to the underlying cause of pneumatosis intestinalis, and this is sometimes difficult to define. Surgical treatment should be considered urgent in symptomatic patients presenting with an acute abdomen, signs of ischemia, or bowel obstruction. In asymptomatic patients with otherwise inconspicuous findings, the underlying disease should be treated first, rather than urgent exploratory surgery considered. Extensive and comprehensive information on the pathophysiology and clinical findings of pneumatosis intestinalis is provided here and is incorporated into a treatment algorithm.
Conclusions: The information presented here allows a better understanding of the radiographic diagnosis and underlying aetiology of pneumatosis intestinalis, and may facilitate the decision-making process in this context, thus providing fast and adequate therapy to particular patients.
Figures
References
-
- DuVernoi JG. Anatomische Beobachtungen der unter der äußeren und inneren Haut der Gederme eingeschlossenen Luft. Phys Med Abbhand Acad Wissensch in Petersb. 1783. p. 182.
-
- Heng Y, Schuffler MD, Haggitt RC, Rohrmann CA. Pneumatosis intestinalis: a review. Am J Gastroenterol. 1995;90:1747–1758. - PubMed
-
- Koss LG. Abdominal gas cysts (pneumatosis cystoides intestinorum hominis): an analysis with a report of a case and a critical review of the literature. AMA Arch Pathol. 1952;53:523–549. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
