

CT assessment of woodworkers' nasal adenocarcinomas confirms the origin in the olfactory cleft
- PMID: 19541776
- PMCID: PMC7051534
- DOI: 10.3174/ajnr.A1648
CT assessment of woodworkers' nasal adenocarcinomas confirms the origin in the olfactory cleft
Abstract
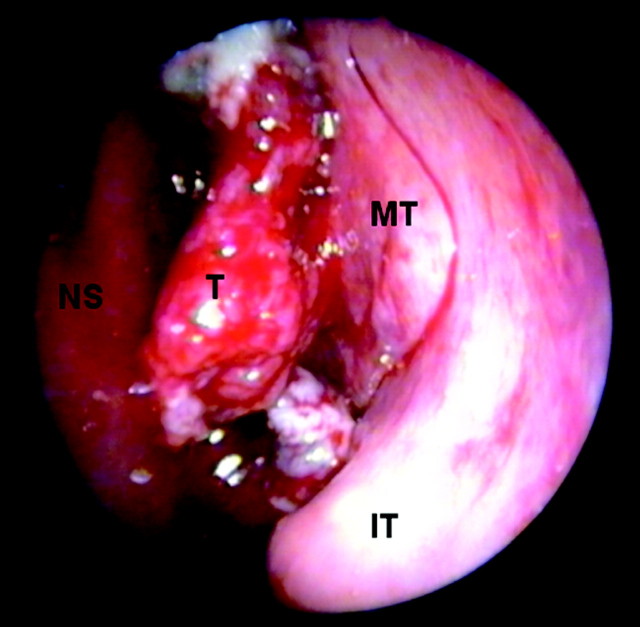
Background and purpose: Endoscopic endonasal surgery let us observe that woodworkers' nasal adenocarcinomas originate in the olfactory cleft. Our aim was the identification of CT imaging features that corroborate the olfactory cleft as the site of origin for woodworkers' adenocarcinoma.
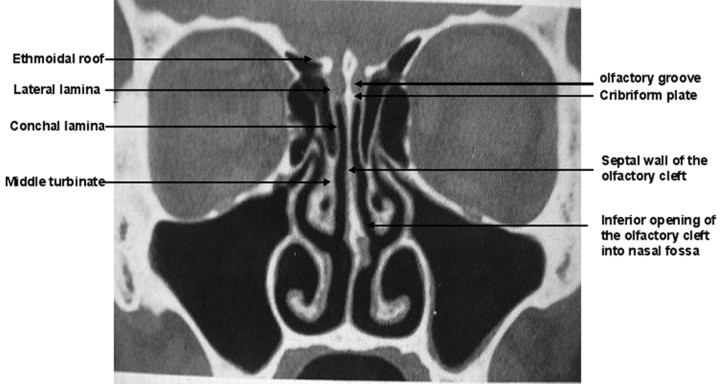
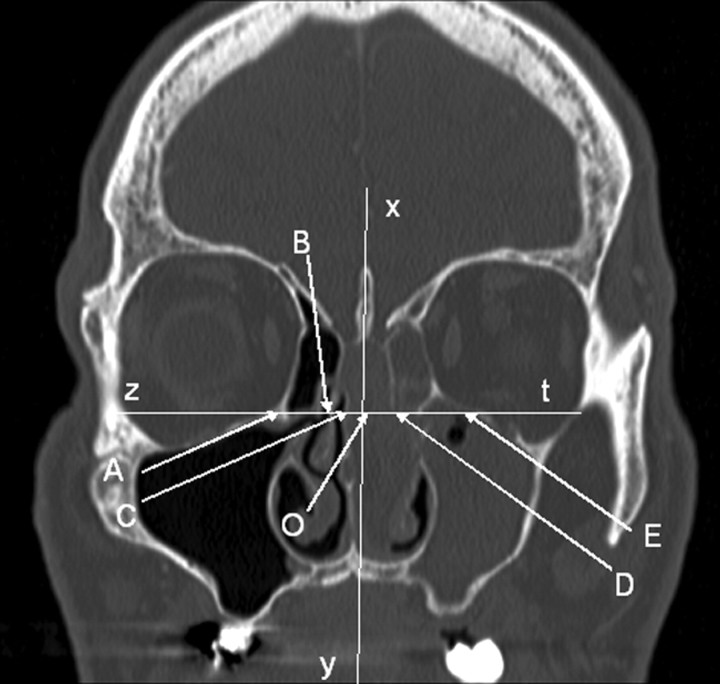
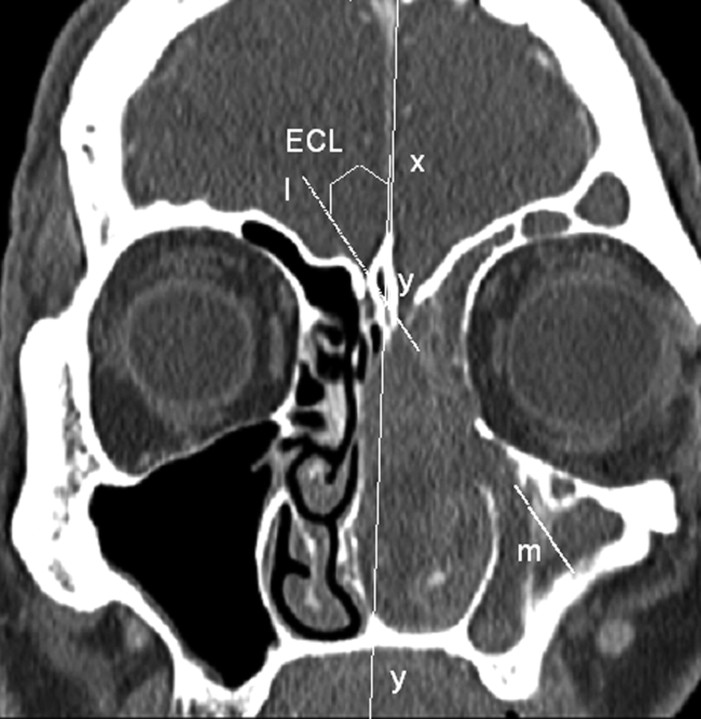
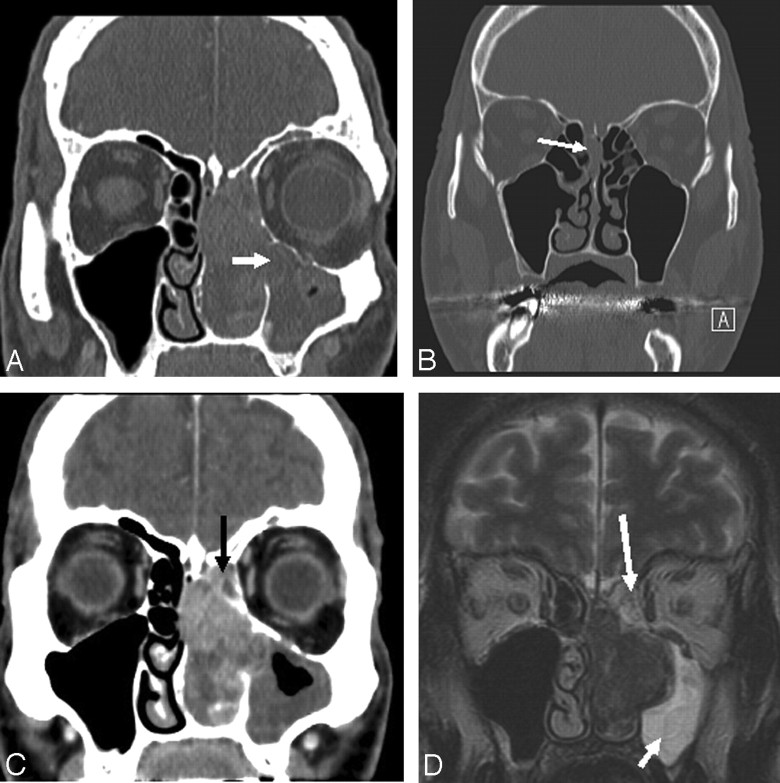
Materials and methods: We designed a retrospective study to compare CT scans of 27 unilateral olfactory cleft adenocarcinomas with 30 cases of nasosinusal polyposis (NSP) and 33 healthy sinus controls. Enlargement of the olfactory cleft, lateralization of the ethmoidal turbinate wall, and contralateral bulging of the nasal septum were measured on coronal scans passing through crista galli and posterior half of both ocular globes. Comparisons have been performed by using analysis of variance and the Bonferroni procedure.
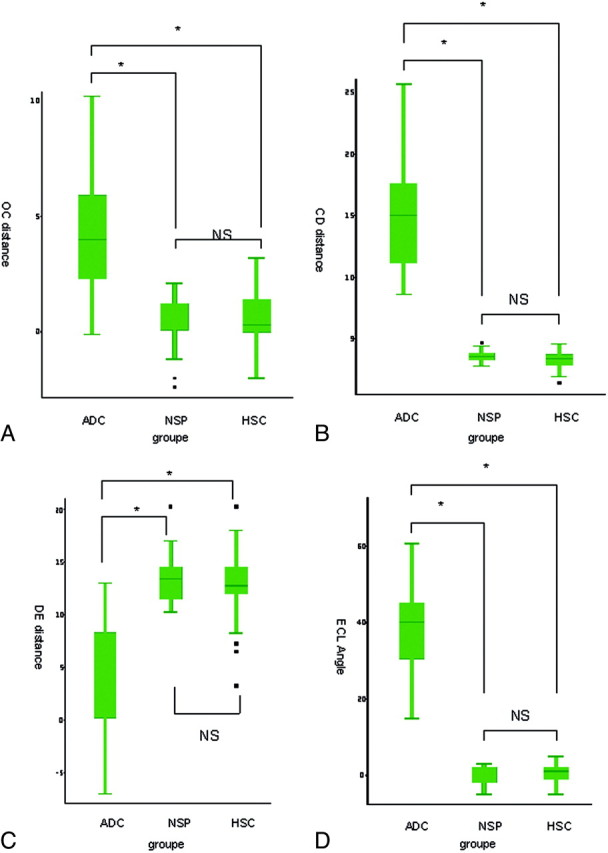
Results: The nasal septum was significantly bulging across the midline in adenocarcinoma (4.6 +/- 3 mm; range, -0.1-13.7 mm) compared with NSP (0.7 +/- 1 mm; range, -2.1-2.3 mm) or healthy sinus controls (0.5 +/- 1 mm; range, -1.2-2 mm) (P < .001). The olfactory cleft was significantly wider in adenocarcinoma (15.1 +/- 4.5 mm; range, 8.6-25.7 mm) than in NSP (3.6 +/- 0.4 mm; range, 2.8-4.6 mm) or healthy sinus controls (3.3 +/- 0.7 mm; range, 1.4-4.6 mm). The ethmoidal labyrinth width was significantly smaller on the pathologic side in adenocarcinoma (7.2 +/- 2.7 mm; range, 3.2-14.2 mm) than in the control groups (P < .001). Whereas the angle between the conchal lamina and vertical midline was close to zero degrees in NSP (0.03 +/- 2.25 degrees ; range, -5 degrees -3 degrees ) and healthy sinus controls (0.45 +/- 2.13 degrees , range, -5 degrees -5 degrees ), it reached 39.76 +/- 13.83 degrees (P < .001) in adenocarcinoma.
Conclusions: Radiologists should suspect nasal adenocarcinoma on sinus CT scans showing a unilateral expanding opacity of the olfactory cavity.
Figures
Similar articles
-
Endoscopic surgery reveals that woodworkers' adenocarcinomas originate in the olfactory cleft.Rhinology. 2007 Dec;45(4):308-14. Rhinology. 2007. PMID: 18085026
-
Cribriform Plate, Crista Galli, Olfactory Fossa and Septal Deviation.Curr Med Imaging Rev. 2019;15(3):319-325. doi: 10.2174/1573405614666180314150237. Curr Med Imaging Rev. 2019. PMID: 31989883
-
[Woodworker's nasal adenocarcinoma revealed by anosmia].Ann Otolaryngol Chir Cervicofac. 2009 Mar;126(1):6-10. doi: 10.1016/j.aorl.2009.01.002. Epub 2009 Feb 18. Ann Otolaryngol Chir Cervicofac. 2009. PMID: 19232569 French.
-
Current status and new developments in techniques for imaging the nose and sinuses.Otolaryngol Clin North Am. 1997 Jun;30(3):371-87. Otolaryngol Clin North Am. 1997. PMID: 9162123 Review.
-
Survey anatomy and histological observation of the nasal cavity of Tupaia belangeri chinensis (Tupaiidae, Scandentia, Mammalia).Anat Rec (Hoboken). 2022 Jun;305(6):1448-1458. doi: 10.1002/ar.24793. Epub 2021 Oct 12. Anat Rec (Hoboken). 2022. PMID: 34605617 Review.
Cited by
-
PET/CT Imaging in Treatment Planning and Surveillance of Sinonasal Neoplasms.Cancers (Basel). 2023 Jul 25;15(15):3759. doi: 10.3390/cancers15153759. Cancers (Basel). 2023. PMID: 37568575 Free PMC article. Review.
-
Choice of surgery in intestinal-type adenocarcinoma of the sinonasal tract: a long-term comparative study.Eur Arch Otorhinolaryngol. 2024 Jun;281(6):2993-3004. doi: 10.1007/s00405-024-08447-w. Epub 2024 Jan 16. Eur Arch Otorhinolaryngol. 2024. PMID: 38228884
-
Sinonasal carcinoma: clinical, pathological, genetic and therapeutic advances.Nat Rev Clin Oncol. 2014 Aug;11(8):460-72. doi: 10.1038/nrclinonc.2014.97. Epub 2014 Jun 17. Nat Rev Clin Oncol. 2014. PMID: 24935016 Review.
-
Imaging of sinonasal tumours.Cancer Imaging. 2012 May 7;12:136-52. doi: 10.1102/1470-7330.2012.0015. Cancer Imaging. 2012. PMID: 22571851 Free PMC article. Review.
-
Sensory Changes Following the Lateral Nasal Wall Surgery: A Systematic Review.Cureus. 2024 Dec 13;16(12):e75628. doi: 10.7759/cureus.75628. eCollection 2024 Dec. Cureus. 2024. PMID: 39803144 Free PMC article. Review.
References
-
- Klintenberg C, Olofsson J, Hellquist H, et al. Adenocarcinoma of the ethmoid sinuses: a review of 28 cases with special reference to wood dust exposure. Cancer 1984;54:482–88 - PubMed
-
- Howard DJ, Lund VJ, Wei WI. Craniofacial resection for tumors of the nasal cavity and paranasal sinuses: a 25-year experience. Head Neck 2006;28:867–73 - PubMed
-
- Goffart Y, Jorissen M, Daele J, et al. Minimally invasive endoscopic management of malignant sinonasal tumours. Acta Otorhinolaryngol Belg 2000;54:221–32 - PubMed
-
- Lund V, Howard DJ, Wei WI. Endoscopic resection of malignant tumors of the nose and sinuses. Am J Rhinol 2007;21:89–94 - PubMed
-
- Jankowski R, Georgel T, Vignaud JM, et al. Endoscopic surgery reveals that woodworkers’ adenocarcinomas originate in the olfactory cleft. Rhinology 2007;45:308–14 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical