

Cigarette smoking is associated with subclinical parenchymal lung disease: the Multi-Ethnic Study of Atherosclerosis (MESA)-lung study
- PMID: 19542480
- PMCID: PMC2742759
- DOI: 10.1164/rccm.200812-1966OC
Cigarette smoking is associated with subclinical parenchymal lung disease: the Multi-Ethnic Study of Atherosclerosis (MESA)-lung study
Abstract
Rationale: Cigarette smoking is a risk factor for diffuse parenchymal lung disease. Risk factors for subclinical parenchymal lung disease have not been described.
Objectives: To determine if cigarette smoking is associated with subclinical parenchymal lung disease, as measured by spirometric restriction and regions of high attenuation on computed tomography (CT) imaging.
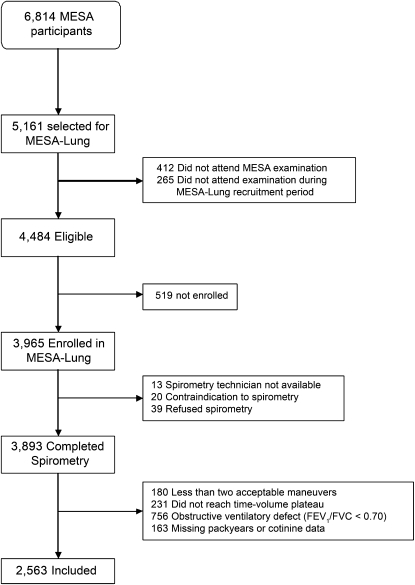
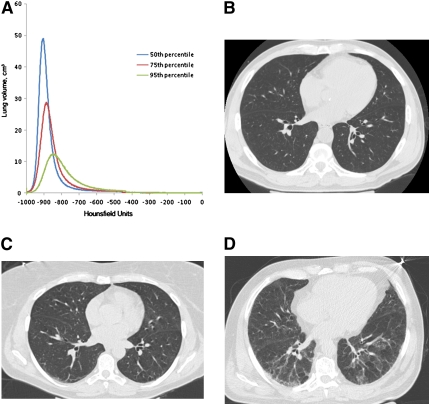
Methods: We examined 2,563 adults without airflow obstruction or clinical cardiovascular disease in the Multi-Ethnic Study of Atherosclerosis, a population-based cohort sampled from six communities in the United States. Cumulative and current cigarette smoking were assessed by pack-years and urine cotinine, respectively. Spirometric restriction was defined as a forced vital capacity less than the lower limit of normal. High attenuation areas on the lung fields of cardiac CT scans were defined as regions having an attenuation between -600 and -250 Hounsfield units, reflecting ground-glass and reticular abnormalities. Generalized additive models were used to adjust for age, gender, race/ethnicity, smoking status, anthropometrics, center, and CT scan parameters.
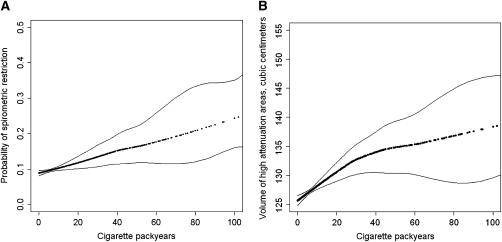
Measurements and main results: The prevalence of spirometric restriction was 10.0% (95% confidence interval [CI], 8.9-11.2%) and increased relatively by 8% (95% CI, 3-12%) for each 10 cigarette pack-years in multivariate analysis. The median volume of high attenuation areas was 119 cm(3) (interquartile range, 100-143 cm(3)). The volume of high attenuation areas increased by 1.6 cm(3) (95% CI, 0.9-2.4 cm(3)) for each 10 cigarette pack-years in multivariate analysis.
Conclusions: Smoking may cause subclinical parenchymal lung disease detectable by spirometry and CT imaging, even among a generally healthy cohort.
Figures
Similar articles
-
Smoking and Subclinical ILD in RA versus the Multi-Ethnic Study of Atherosclerosis.PLoS One. 2016 Apr 6;11(4):e0153024. doi: 10.1371/journal.pone.0153024. eCollection 2016. PLoS One. 2016. PMID: 27050433 Free PMC article.
-
Serum 25-Hydroxyvitamin D Concentrations Are Associated with Computed Tomography Markers of Subclinical Interstitial Lung Disease among Community-Dwelling Adults in the Multi-Ethnic Study of Atherosclerosis (MESA).J Nutr. 2018 Jul 1;148(7):1126-1134. doi: 10.1093/jn/nxy066. J Nutr. 2018. PMID: 29931068 Free PMC article.
-
The association of pipe and cigar use with cotinine levels, lung function, and airflow obstruction: a cross-sectional study.Ann Intern Med. 2010 Feb 16;152(4):201-10. doi: 10.7326/0003-4819-152-4-201002160-00004. Ann Intern Med. 2010. PMID: 20157134 Free PMC article.
-
[The relationship between cigarette smoking and some types of idiopathic interstitial pneumonias].Wiad Lek. 2008;61(1-3):48-52. Wiad Lek. 2008. PMID: 18717043 Review. Polish.
-
Legacy of MESA.Glob Heart. 2016 Sep;11(3):269-274. doi: 10.1016/j.gheart.2016.08.004. Glob Heart. 2016. PMID: 27741974 Free PMC article. Review.
Cited by
-
Smoking and Subclinical ILD in RA versus the Multi-Ethnic Study of Atherosclerosis.PLoS One. 2016 Apr 6;11(4):e0153024. doi: 10.1371/journal.pone.0153024. eCollection 2016. PLoS One. 2016. PMID: 27050433 Free PMC article.
-
Characteristics of Current Smokers versus Former Smokers with COPD and Their Associations with Smoking Cessation Within 4.5 Years: Results from COSYCONET.Int J Chron Obstruct Pulmon Dis. 2023 Dec 6;18:2911-2923. doi: 10.2147/COPD.S436669. eCollection 2023. Int J Chron Obstruct Pulmon Dis. 2023. PMID: 38084341 Free PMC article.
-
Assessing predictors of rheumatoid arthritis-associated interstitial lung disease using quantitative lung densitometry.Rheumatology (Oxford). 2022 Jul 6;61(7):2792-2804. doi: 10.1093/rheumatology/keab828. Rheumatology (Oxford). 2022. PMID: 34747452 Free PMC article.
-
Identification and Remediation of Environmental Exposures in Patients With Interstitial Lung Disease: Evidence Review and Practical Considerations.Chest. 2021 Jul;160(1):219-230. doi: 10.1016/j.chest.2021.02.021. Epub 2021 Feb 18. Chest. 2021. PMID: 33609518 Free PMC article. Review.
-
MUC5B promoter polymorphism and interstitial lung abnormalities.N Engl J Med. 2013 Jun 6;368(23):2192-200. doi: 10.1056/NEJMoa1216076. Epub 2013 May 21. N Engl J Med. 2013. PMID: 23692170 Free PMC article.
References
-
- American Thoracic Society/European Respiratory Society. International multidisciplinary consensus classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med 2002;165:277–304. - PubMed
-
- American Thoracic Society/European Respiratory Society. Idiopathic pulmonary fibrosis: diagnosis and treatment. International consensus statement. Am J Respir Crit Care Med 2000;161:646–664. - PubMed
-
- King TE Jr, Tooze JA, Schwarz MI, Brown KR, Cherniack RM. Predicting survival in idiopathic pulmonary fibrosis: scoring system and survival model. Am J Respir Crit Care Med 2001;164:1171–1181. - PubMed
-
- Carrington CB, Gaensler EA, Coutu RE, FitzGerald MX, Gupta RG. Natural history and treated course of usual and desquamative interstitial pneumonia. N Engl J Med 1978;298:801–809. - PubMed
-
- Fraig M, Shreesha U, Savici D, Katzenstein AL. Respiratory bronchiolitis: a clinicopathologic study in current smokers, ex-smokers, and never-smokers. Am J Surg Pathol 2002;26:647–653. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
