

Neuropathology-based risk scoring for dementia diagnosis in the elderly
- PMID: 19542615
- PMCID: PMC2852462
- DOI: 10.3233/JAD-2009-1105
Neuropathology-based risk scoring for dementia diagnosis in the elderly
Abstract
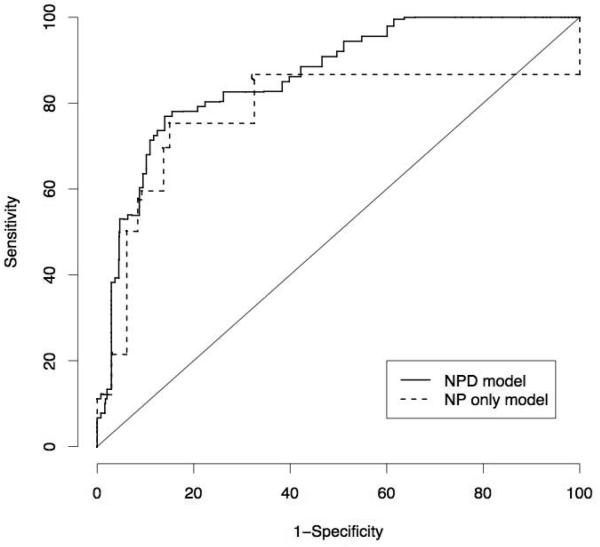
Current neuropathologic consensus criteria for diagnosis of dementia yield a classification of processes that likely contributed to dementia in that individual. While dementia diagnosis currently relies on clinical criteria, practicing neuropathologists and researchers might benefit from a simple, accurate risk scoring protocol for the neuropathologic diagnosis of dementia. Using 232 consecutive autopsies from the population-based Adult Changes in Thought study, we developed two logistic regression-based risk scoring systems; one solely using neuropathologic measures and a second additionally including demographic information. Inverse-probability weighting was used to adjust for inherent selection bias in autopsy-based studies of dementing illnesses. Both systems displayed high levels of predictive accuracy; bias-adjusted area-under-the-curve statistics were 0.78 (95% CI 0.71, 0.85) and 0.87 (95% CI 0.83, 0.92), indicating improved performance with the inclusion of demographic characteristics, specifically age and birth cohort information. Application of the combined neuropathology/demographic model yielded bias-adjusted sensitivity and specificity of 81% each. In contrast, application of NIA-Reagan criteria yielded sensitivity and specificity of 53% and 84%. Our proposed scoring systems provide neuropathologists with tools to make a diagnosis, and interpret their diagnosis in the light of known sensitivity and specificity estimates. Evaluation in independent samples will be important to verify our findings.
Figures
References
-
- Hyman B, Trojanowski J. Consensus recommendations for the postmortem diagnosis of Alzheimer's disease from The National Institute on Aging Reagan Institute Working Group on diagnostic criteria for the neuropathological assessment of Alzheimer's disease. Neurobiol Aging. 1997;18:S1–2. - PubMed
-
- Vinters HV. Surgical pathologic findings of extratemporal-based intractable epilepsy. A study of 133 consecutive cases. Arch Pathol Lab Med. 2000;124:1111–1112. - PubMed
-
- Roman GC, Erkinjuntti T, Wallin A, Pantoni L, Chui HC. Subcortical ischaemic vascular dementia. Lancet Neurol. 2002;1:426–436. - PubMed
-
- Kalaria RN, Kenny RA, Ballard CG, Perry R, Ince P, Polvikoski T. Towards defining the neuropathological substrates of vascular dementia. J Neurol Sci. 2004;226:75–80. - PubMed
-
- Petrovitch H, Ross GW, Steinhorn SC, Abbott RD, Markesbery W, Davis D, Nelson J, Hardman J, Masaki K, Vogt MR, Launer L, White LR. AD lesions and infarcts in demented and non-demented Japanese-American men. Ann Neurol. 2005;57:98–103. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
