

Increased clearance of cortisol by 5beta-reductase in a subgroup of women with adrenal hyperandrogenism in polycystic ovary syndrome
- PMID: 19542736
- PMCID: PMC4425940
- DOI: 10.1007/BF03346454
Increased clearance of cortisol by 5beta-reductase in a subgroup of women with adrenal hyperandrogenism in polycystic ovary syndrome
Abstract
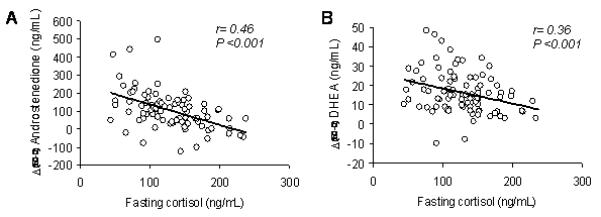
Objective: Increased peripheral metabolism of cortisol may explain compensatory ACTH-dependent adrenal steroidogenesis and hence hyperandrogenism in polycystic ovary syndrome (PCOS). Previous studies have described an increased 5alpha-reduction of cortisol or impaired regeneration of cortisol by 11beta-HSD1 in PCOS. However, these observations may be confounded by obesity. Moreover, the relationship between alterations in cortisol metabolism and the extent of adrenal androgen hyper-secretion in response to ACTH has not been established. This study aimed to examine the association between cortisol metabolism and ACTH-dependent adrenal hyperandrogenism in PCOS, independently of obesity.
Design: We compared 90 PCOS women (age 18-45 yr) stratified by adrenal androgen responses to ACTH1-24 and 45 controls matched for age and body weight.
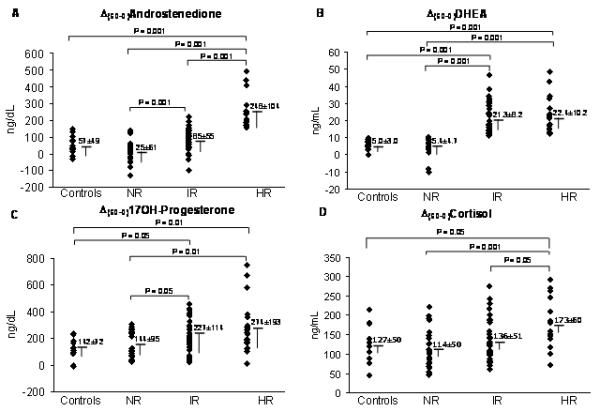
Methods: PCOS women were stratified as normal responders (NR), intermediate responders (IR), and high responders (HR) to 250 microg ACTH1-24: NR (no.=27) had androstenedione and DHEA responses within 2 SD of the mean in controls; IR (no.=43) had DHEA responses >2 SD above controls; HR (no.=20) had both androstenedione and DHEA responses >2 SD above controls.
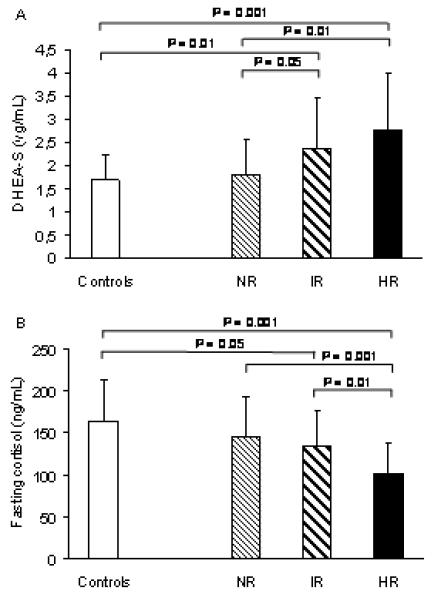
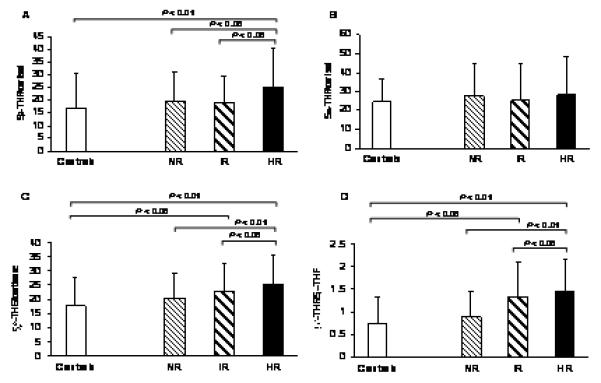
Results: All groups were similar for age, body weight, and body fat distribution. Basal testosterone, androstenedione, and 5alpha-dihydrotestosterone plasma levels were similarly elevated among the 3 groups of PCOS compared with controls, whereas basal DHEA-S was higher in HR (2.8+/-1.2 microg/ml) and IR (2.4+/-1.1 microg/ml) than in NR (1.8+/-0.8 microg/ml) and controls (1.7+/-0.6 microg/ml). The HR group had the lowest basal plasma cortisol levels (101+/-36 ng/ml vs IR 135+/-42 ng/ml, NR 144+/-48 ng/ml, and controls 165+/-48 ng/ml; all p<0.01), but the greatest cortisol response to ACTH1-24 (Delta(60-0)cortisol 173+/-60 ng/ml vs IR 136+/-51 ng/ml, NR 114+/-50 ng/ml, and controls 127+/-50 ng/ml; all p<0.01), and the highest urinary excretion of total and 5beta-reduced cortisol metabolites (eg 5beta-tetrahydrocortisol/ cortisol ratio 25.2+/-15.3 vs IR 18.8+/-10.7, NR 19.7+/-11.4, and controls 17.2+/-13.7; all p<0.05). There were no differences in urinary excretion of 5alpha-reduced cortisol metabolites or in 5alpha-dihydrotestosterone/testosterone ratio between groups.
Conclusions: Adrenal androgen excess in PCOS is associated with increased inactivation of cortisol by 5beta-reductase that may lower cortisol blood levels and stimulate ACTH-dependent steroidogenesis.
Figures
References
-
- Carmina E, Koyama T, Chang L, Stanczyk FZ, Lobo RA. Does ethnicity influence the prevalence of adrenal hyperandrogenism and insulin resistance in polycystic ovary syndrome? Am J Obstet Gynecol. 1992;167:1807–1812. - PubMed
-
- Wild RA, Umstot ED, Andersen RN, Ranney GB, Givens JR. Androgen parameters and their correlation with body weight in one hundred thirty-eight women thought to have hyperandrogenism. Am J Obstet Gynecol. 1983;146:602–605. - PubMed
-
- Hoffman DI, Klove K, Lobo RA. The prevalence and significance of elevated dehydroepiandrosterone sulfate levels in anovulatory women. Fertil Steril. 1984;42:76–81. - PubMed
-
- Azziz R, Black V, Hines GA, Fox LM, Boots LR. Adrenal androgen excess in the polycystic ovary syndrome: sensitivity and responsivity of the hypothalamic-pituitary-adrenal axis. J Clin Endocrinol Metab. 1998;83:2317–2323. - PubMed
-
- Walker BR. Activation of the hypothalamic-pituitary-adrenal axis: cause or consequence? GH & IGF Res. 2001;11(Suppl A):S91–95. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
