

Who's too old to screen? Prostate cancer in elderly men
- PMID: 19543463
- PMCID: PMC2692165
- DOI: 10.5489/cuaj.1071
Who's too old to screen? Prostate cancer in elderly men
Abstract
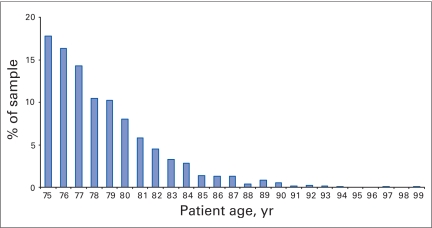
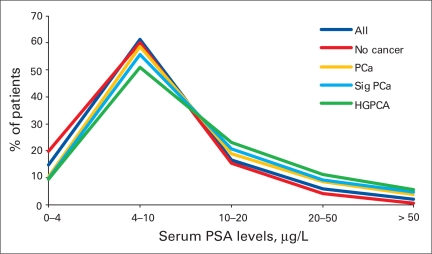
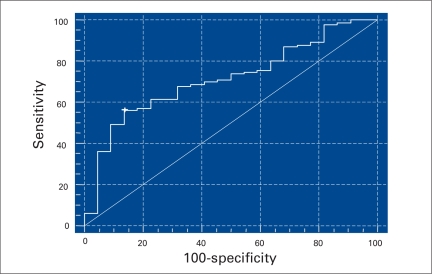
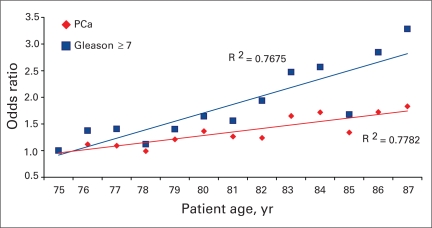
INTRODUCTION: Prostate cancer is the most common nonskin malignancy affecting men and is the second leading cause of cancer-related death in North America. The incidence of prostate cancer increases dramatically with age. However, many health authorities advocate the cessation of routine prostate cancer testing in men older than 75 because of the belief that most patients will have a clinically insignificant cancer and will not benefit from therapy. The true prevalence of clinically significant prostate cancer in elderly men is not known. METHODS: We analyzed 1446 needle biopsies of the prostate in men aged 75 or older. All pathological reviews were conducted by the pathology department at the Methodist Hospital in Houston, Tex. Data were collected from pathology reports, hospital and clinic databases, and medical records when available. Data obtained included age at biopsy, serum prostate-specific antigen (PSA) levels, number of positive core biopsies and Gleason grade. Statistical analysis was performed using Stata. Clinically significant cancer was defined by the pathological presence of Gleason grade 6 adenocarcinoma in more than 1 biopsy core or the presence of any Gleason 4 or 5 component in the biopsy. RESULTS: The median age of the patients included in the study was 78.8 and 95% of the patients were between the ages of 75 and 85. The mean serum PSA level for patients biopsied was 10.4 mug/L. Of all biopsies reviewed, 53% were positive for prostate cancer and 78% of these would be defined as clinically significant cancer. Regression analysis revealed age to be a significant (p < 0.05) factor for increased Gleason grade in positive biopsies. Logistic regression revealed age as a significant factor (p < 0.05) for clinically significant prostate cancer even when controlling for PSA. A serum PSA threshold value of 6.5 mug/L would have missed 38% of significant cancers and a threshold of 4.0 mug/L would have missed 8% of significant cancers. CONCLUSION: Our findings suggest that the prevalence of clinically significant prostate cancer in the elderly population may be higher than previously thought. As the population continues to live longer and healthier lives, it will become more common to confront prostate cancer morbidity in the eldery population. Using higher serum PSA thresholds to eliminate unnecessary biopsies in older men does not appear to help identify patients at greater risk of having clinically significant prostate cancer. Patients with prostate cancer having aggressive clinical features may benefit from treatment of their prostate cancer well into their eighth and ninth decades of life. Testing and diagnostic recommendations should reflect the potential benefit of identifying patients with aggressive prostate cancer even after age 75.
Introduction :: Le cancer de la prostate est le type de cancer non cutané le plus fréquent chez les hommes et la seconde cause de décès lié au cancer en importance en Amérique du Nord. L’incidence du cancer de la prostate augmente grandement avec l’âge. Néanmoins, de nombreuses autorités en matière de santé avancent l’idée de mettre fin au dépistage systématique du cancer de la prostate chez les hommes de plus de 75 ans en raison de la croyance selon laquelle la plupart des patients présenteront un cancer non significatif sur le plan clinique et ne bénéficieront pas d’un traitement. La véritable prévalence des cas de cancer de la prostate cliniquement significatif chez les hommes âgés n’est pas établie.
Méthodes :: Nous avons analysé 1446 échantillons de biopsie à l’aiguille prélevés au niveau de la prostate chez des patients de 75 ans ou plus. Toutes les analyses de pathologie ont été effectuées par le service de pathologie du Methodist Hospital de Houston, au Texas. Les données ont été tirées des rapports de pathologie, des bases de données des hôpitaux et des cliniques, et des dossiers médicaux lorsque possible. Les données obtenues incluaient l’âge au moment de la biopsie, les valeurs d’antigène prostatique spécifique (APS), le nombre de microbiopsies positives et le score de Gleason. Les analyses statistiques ont été effectuées à l’aide du système Stata. Le cancer cliniquement significatif est défini comme la présence d’un adénocarcinome avec un score de Gleason de 6 dans plus d’une zone de biopsie ou un score de Gleason de 4 ou 5 dans toute partie de l’échantillon.
Résultats :: L’âge moyen des patients inclus était de 78,8 ans et 95 % des patients avaient entre 75 et 85 ans. La valeur moyenne de l’APS chez les patients ayant subi une biopsie était de 10,4 μg/L. De tous les échantillons examinés, 53 % confirmaient la présence d’un cancer de la prostate, et le cancer était défini comme étant cliniquement significatif dans 78 % de ces cas. Une analyse de régression a révélé que l’âge était un facteur significatif (p < 0,05) lié à un score de Gleason plus élevé dans les biopsies positives. Une analyse de régression logistique a révélé que l’âge était aussi un facteur significatif (p < 0,05) lié à un cancer de la prostate cliniquement significatif même en tenant compte du taux d’APS. Une valeur seuil d’APS de 6,5 μg/L serait passée à côté de 38 % des cas de cancer significatif, alors qu’une valeur seuil d’APS de 4,0 μg/L serait passée à côté de 8 % des cancers significatifs.
Conclusion :: Nos observations portent à croire que la prévalence du cancer de la prostate significatif sur le plan clinique chez les patients âgés pourrait être plus élevée qu’on le croit. Avec l’augmentation de l’espérance de vie, l’incidence de la morbidité liée au cancer de la prostate augmentera. Le recours à des valeurs seuils d’APS plus élevées pour éliminer les cas de biopsies non nécessaires chez les hommes âgés ne semble pas aider à cerner les patients présentant un risque plus élevé de cancer de la prostate cliniquement significatif. Les patients atteints de cancer de la prostate cliniquement agressif peuvent bénéficier d’un traitement contre le cancer même lorsqu’ils dépassent largement les 80 ou les 90 ans. Les recommandations concernant le dépistage et le diagnostic devraient refléter les avantages potentiels liés au dépistage d’un cancer de la prostate agressif, même après 75 ans.
Figures

Comment in
- Can Urol Assoc J. 3:211.
Similar articles
-
Prostate gland biopsies and prostatectomies: an Ontario community hospital experience.Can Urol Assoc J. 2008 Oct;2(5):518-23. doi: 10.5489/cuaj.920. Can Urol Assoc J. 2008. PMID: 18953449 Free PMC article.
-
Usefulness of prostate-specific antigen (PSA) rise as a marker of prostate cancer in men treated with dutasteride: lessons from the REDUCE study.BJU Int. 2012 Apr;109(8):1162-9. doi: 10.1111/j.1464-410X.2011.10373.x. Epub 2011 Jun 23. BJU Int. 2012. PMID: 21699645 Clinical Trial.
-
Prostate cancer screening using a combination of risk-prediction, MRI, and targeted prostate biopsies (STHLM3-MRI): a prospective, population-based, randomised, open-label, non-inferiority trial.Lancet Oncol. 2021 Sep;22(9):1240-1249. doi: 10.1016/S1470-2045(21)00348-X. Epub 2021 Aug 13. Lancet Oncol. 2021. PMID: 34391509 Clinical Trial.
-
Prostate biopsy: who, how and when. An update.Can J Urol. 2005 Feb;12 Suppl 1:44-8; discussion 99-100. Can J Urol. 2005. PMID: 15780165 Review.
-
Most prostate cancers missed by raising the upper limit of normal prostate-specific antigen for men in their sixties are clinically significant.Urology. 1998 Dec;52(6):1064-9. doi: 10.1016/s0090-4295(98)00366-5. Urology. 1998. PMID: 9836555 Review.
Cited by
-
Predicting Life Expectancy in Men Diagnosed with Prostate Cancer.Eur Urol. 2015 Nov;68(5):756-65. doi: 10.1016/j.eururo.2015.03.020. Epub 2015 Mar 26. Eur Urol. 2015. PMID: 25819724 Free PMC article. Review.
-
Remaining Life Expectancy Measurement and PSA Screening of Older Men.J Geriatr Oncol. 2012 Jul 1;3(3):196-204. doi: 10.1016/j.jgo.2012.02.003. J Geriatr Oncol. 2012. PMID: 22773938 Free PMC article.
-
Is there ageism in prostate cancer detection?Can Urol Assoc J. 2009 Jun;3(3):211-212. doi: 10.5489/cuaj.1072. Can Urol Assoc J. 2009. PMID: 19543464 Free PMC article. No abstract available.
-
Challenging the 10-year rule: The accuracy of patient life expectancy predictions by physicians in relation to prostate cancer management.Can Urol Assoc J. 2012 Oct;6(5):367-73. doi: 10.5489/cuaj.11161. Can Urol Assoc J. 2012. PMID: 23093629 Free PMC article.
References
-
- American Cancer Society . Cancer facts & figures. 2003. Available: www.cancer.org/downloads/STT/CAFF2003PWSecured.pdf (accessed 2009 Apr 28).
-
- Lu-Yao G, Stukel TA, Yao SL. Prostate-specific antigen screening in elderly men. J Natl Cancer Inst. 2003;95:1792–7. - PubMed
-
- U. S. Preventive Services Task Force Screening for prostate cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2008;149:185–91. - PubMed
-
- Lin K, Lipsitz R, Miller T, et al. Benefits and harms of prostate-specific antigen screening for prostate cancer: an evidence update for the U.S. Preventive Services Task Force. Ann Intern Med. 2008;149:192–9. - PubMed
-
- Noguchi M, Stamey TA, McNeal JE, et al. Relationship between systematic biopsies and histological features of 222 radical prostatectomy specimens: lack of prediction of tumor significance for men with nonpalpable prostate cancer. J Urol. 2001;166:104–9. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
