

Review
doi: 10.1161/HYPERTENSIONAHA.109.133777.
Epub 2009 Jun 22.
Protective importance of the myogenic response in the renal circulation
Affiliations
- PMID: 19546375
- PMCID: PMC2777749
- DOI: 10.1161/HYPERTENSIONAHA.109.133777
Item in Clipboard
Review
Protective importance of the myogenic response in the renal circulation
Hypertension.
2009 Aug.
No abstract available
Conflict of interest statement
Figures
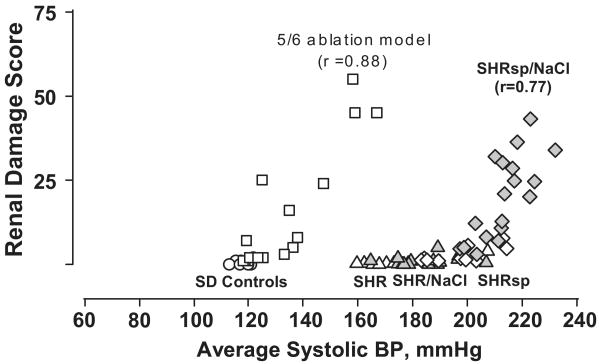
Relationship between renal injury and systolic BP in rat models with intact autoregulation (normotensive Sprague-Dawley [SAD; circles]; spontaneously hypertensive rat [SHR, triangles]; stroke-prone SHR [SHRsp, diamonds]; SHR [gray triangles] and SHRsp [gray diamonds] placed on increased dietary salt intake) and in the 5/6 remnant kidney model [squares], with impaired autoregulation. The renal damage score represents a composite of vascular and glomerular damage scores in the SHRsp and % GS in the 5/6 ablation model. Patterns of injury parallel that of renal autoregulation. The remnant kidney exhibits impaired autoregulation, and exhibits a much lower BP threshold for hypertensive injury than SHR and SHRsp kidneys. (Reprinted with permission from Reference #13 with data reproduced with permission from references #10, and #11).
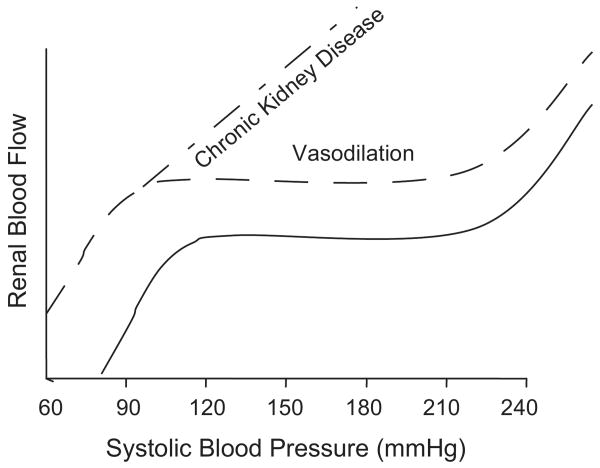
Renal autoregulatory response patterns (‘steady-state’ RBF after step changes in blood pressure) in normal rats with intact renal mass, with vasodilation but preserved autoregulation such as after uninephrectomy, and in the 5/6 renal ablation model of chronic kidney disease (vasodilation and impaired autoregulation). (Reprinted with permission from reference #4).
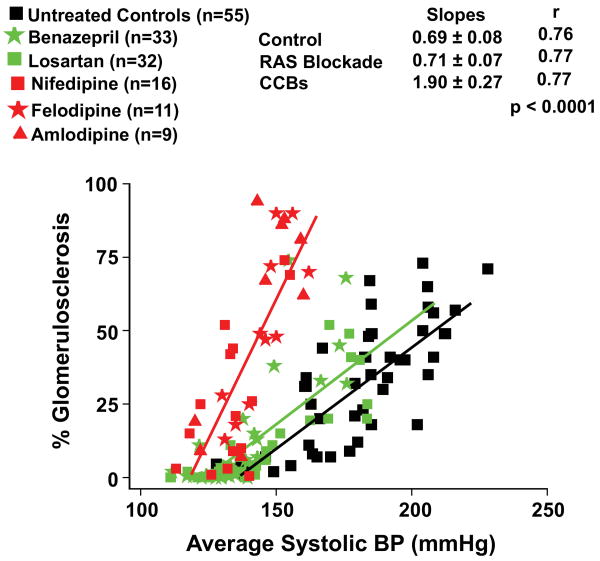
Quantitative relationships between BP and GS in rats with 5/6 renal ablation which had been left untreated or had received dihydropyridine calcium channel blockers (DHP CCBs) for 7 weeks (data from references #23-25). For comparison, data are also shown for rats with 5/6 ablation who had been similarly treated with renin-angiotensin systems (RAS) blockade with either the ACE inhibitor, benazepril or the AT1 receptor blocker, losartan. The doses of benazepril used were 25, 50 or 100 mg/L and of losartan 50, 120 or 180 mg/L of drinking water (data from reference #27). Note the significant adverse effects of the DHP CCBs as compared to untreated and RAS blockade treated rats on the slope of the relationship between average systolic BP and % GS (increase in % GS/mmHg increase in systolic BP) (reprinted with permission from reference #4).
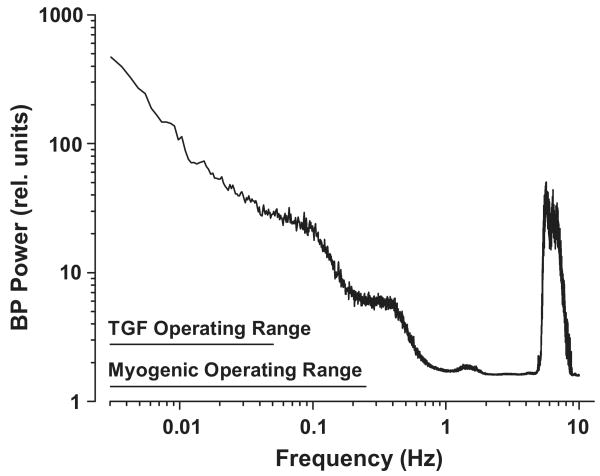
Blood pressure (BP) power spectrum in the conscious rat (mean data, n=10). The BP signal is a complex wave form derived from various fluctuations occurring at different frequencies. BP power is proportional to the square of the amplitude of these fluctuations (from the mean BP) and is plotted as a function of oscillation frequency (f). Note the 1/f relationship seen at frequencies below 1 Hz and the natural frequencies of TGF and the myogenic response. A major BP power peak is produced at the heart rate frequency (6 Hz in the rat). By current interpretations, this signal is beyond the myogenic operating range and, accordingly, is handled passively by the renal vasculature. (Reprinted with permission from Reference #13).
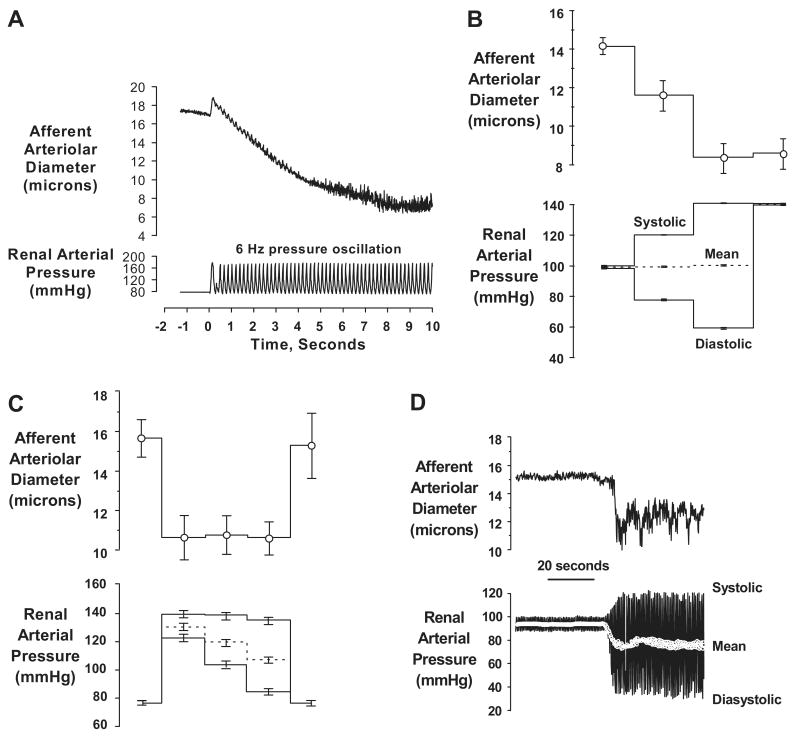
Data illustrating the afferent arteriolar responses in the rat hydronephrotic rat kidney preparation to pressure inputs using high speed video analysis. Note, all pressures are measured within the renal artery. (a) A tracing illustrating the sustained afferent arteriolar vasoconstriction elicited by pressure oscillations presented at the rat heart rate (6 Hz). (b) afferent arteriole responds to increase in peak pressure signal (systolic) even when mean perfusion pressure is maintained constant (n=10). (c) myogenic tone established by submaximal increase in systolic (peak) pressure signal is not altered when mean pressure is reduced by marked reductions in the nadir (diastolic) pressure (n=7). (d) tracing illustrating the afferent arteriolar response to changes in the oscillating pressure signal. Note that modest increase in systolic BP evokes vasoconstriction even though mean pressure is reduced. (Reprinted with permission from reference #13 and #32).
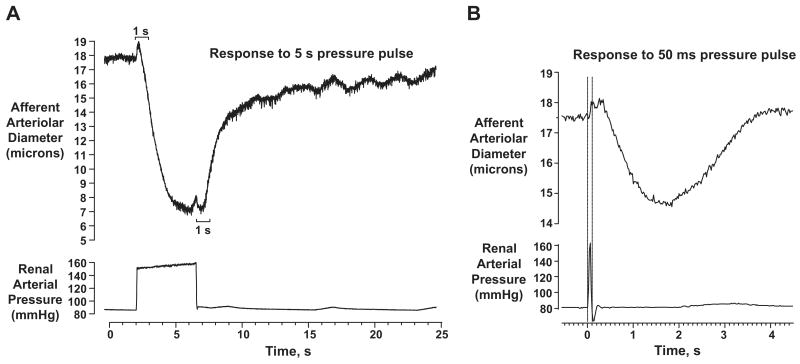
(a) Illustration of the kinetic features of the afferent arteriolar myogenic response in the hydronephrotic kidney preparation to a step change in pressure. Note, the very short “delay” in onset of vasoconstriction (200-300 ms) and a much longer “delay” in onset of relaxation (∼1 sec). (b) The afferent arteriolar vasoconstriction response to a 50 msec pressure pulse. Note that once initiated, events proceed during these “delay” periods.
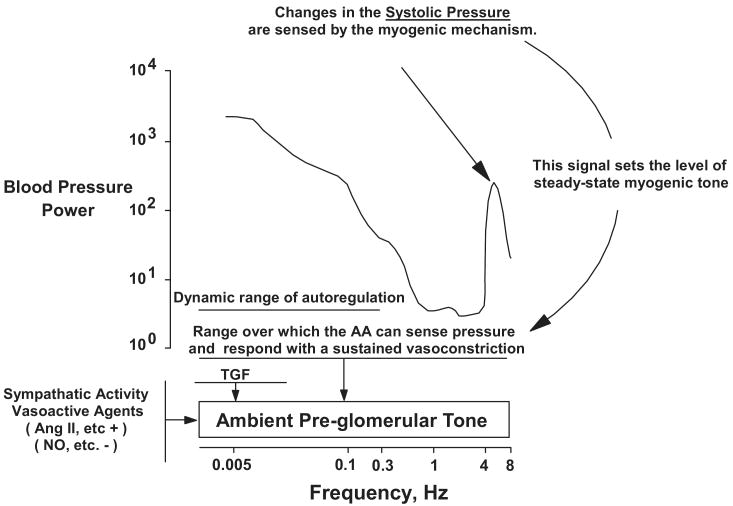
Proposed model of pressure-induced activation of the renal vasculature. Changes in the oscillating systolic pressure are sensed by the myogenic mechanism and it is this signal that sets the level of steady-state myogenic tone. This response provides protection over the full range of BP frequencies by limiting the transmission of pressure transients to the glomerular capillaries. Dynamic autoregulation of RBF and GFR occurs at frequencies below the myogenic operating range as a consequence of this myogenic response and, at lower frequencies, as mediated by TGF. AA, afferent arteriole. (Reprinted with permission from reference #13).
References
-
- US Renal Data System: USRDS 2005 Annual Data Report, Atlas of End Stage Renal Disease in the United States. Bethesda, MD: National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health; 2005.
-
- Bidani AK, Griffin KA. Long-term renal consequences of hypertension for normal and diseased kidneys. Curr Opin Nephrol Hypertens. 2002;11:73–80. - PubMed
-
- Bidani AK, Griffin KA. Pathophysiology of hypertensive renal damage: implications for therapy. Hypertens. 2004;44:1–7. - PubMed
-
- Griffin KA, Bidani AK. Progression of renal disease: the renoprotective specificity of renin angiotensin system blockade. Clin J Am Soc Nephrol. 2006;1:1054–1065. invited review. - PubMed
-
- Olson JL. Renal Disease caused by hypertension. In: Jennette JC, Olson JL, Schwartz MM, Silva FG, editors. Heptinstall's Pathology of the Kidney. sixth. II. Lippincott Williams & Wilkins; Philadelphia, PA: 2006. pp. 937–990.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
