

Cost-effectiveness of total knee arthroplasty in the United States: patient risk and hospital volume
- PMID: 19546411
- PMCID: PMC2731300
- DOI: 10.1001/archinternmed.2009.136
Cost-effectiveness of total knee arthroplasty in the United States: patient risk and hospital volume
Abstract
Background: Total knee arthroplasty (TKA) relieves pain and improves quality of life for persons with advanced knee osteoarthritis. However, to our knowledge, the cost-effectiveness of TKA and the influences of hospital volume and patient risk on TKA cost-effectiveness have not been investigated in the United States.
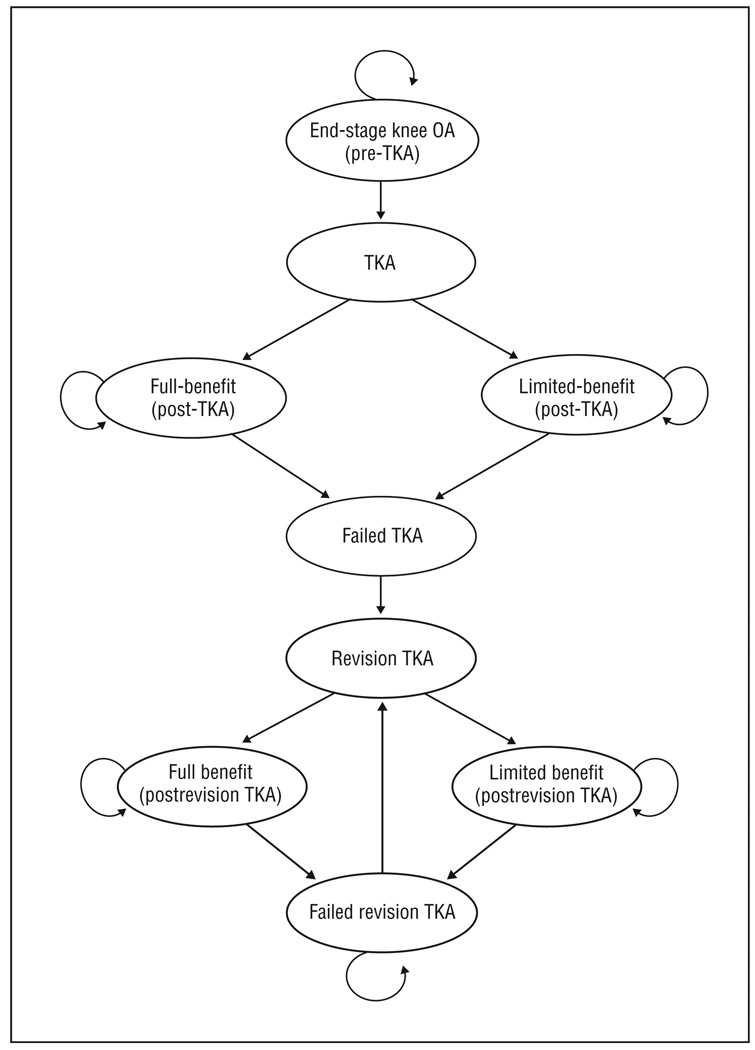
Methods: We developed a Markov, state-transition, computer simulation model and populated it with Medicare claims data and cost and outcomes data from national and multinational sources. We projected lifetime costs and quality-adjusted life expectancy (QALE) for different risk populations and varied TKA intervention and hospital volume. Cost-effectiveness of TKA was estimated across all patient risk and hospital volume permutations. Finally, we conducted sensitivity analyses to determine various parameters' influences on cost-effectiveness.
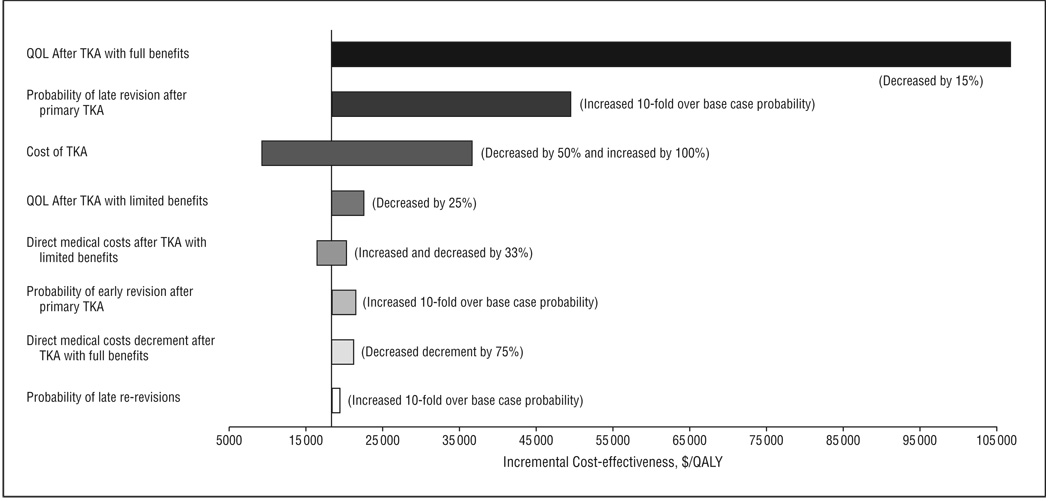
Results: Overall, TKA increased QALE from 6.822 to 7.957 quality-adjusted life years (QALYs). Lifetime costs rose from $37,100 (no TKA) to $57 900 after TKA, resulting in an incremental cost-effectiveness ratio of $18,300 per QALY. For high-risk patients, TKA increased QALE from 5.713 to 6.594 QALY, yielding a cost-effectiveness ratio of $28,100 per QALY. At all risk levels, TKA was more costly and less effective in low-volume centers than in high-volume centers. Results were insensitive to variations of key input parameters within policy-relevant, clinically plausible ranges. The greatest variations were seen for the quality of life gain after TKA and the cost of TKA.
Conclusions: Total knee arthroplasty appears to be cost-effective in the US Medicare-aged population, as currently practiced across all risk groups. Policy decisions should be made on the basis of available local options for TKA. However, when a high-volume hospital is available, TKAs performed in a high-volume hospital confer even greater value per dollar spent than TKAs performed in low-volume centers.
Figures
Comment in
-
Cost-effectiveness analysis of an established, effective procedure.Arch Intern Med. 2009 Jun 22;169(12):1102-3. doi: 10.1001/archinternmed.2009.144. Arch Intern Med. 2009. PMID: 19546409 No abstract available.
References
-
- Dillon CF, Rasch EK, Gu Q, Hirsch R. Prevalence of knee osteoarthritis in the United States: arthritis data from the Third National Health and Nutrition Examination Survey 1991–94. J Rheumatol. 2006;33(11):2271–2279. - PubMed
-
- Gabriel SE, Crowson CS, Campion ME, O’Fallon WM. Direct medical costs unique to people with arthritis. J Rheumatol. 1997;24(4):719–725. - PubMed
-
- Lanes SF, Lanza LL, Radensky PW, et al. Resource utilization and cost of care for rheumatoid arthritis and osteoarthritis in a managed care setting: the importance of drug and surgery costs. Arthritis Rheum. 1997;40(8):1475–1481. - PubMed
-
- Clarfield AM. Teaching public health related to the elderly. Public Health Rev. 2002;30(1–4):271–276. - PubMed
-
- Elders MJ. The increasing impact of arthritis on public health. J Rheumatol Suppl. 2000;60:6–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
