

Nocturnal Arrhythmias across a spectrum of obstructive and central sleep-disordered breathing in older men: outcomes of sleep disorders in older men (MrOS sleep) study
- PMID: 19546416
- PMCID: PMC2802061
- DOI: 10.1001/archinternmed.2009.138
Nocturnal Arrhythmias across a spectrum of obstructive and central sleep-disordered breathing in older men: outcomes of sleep disorders in older men (MrOS sleep) study
Abstract
Background: Rates of cardiac arrhythmias increase with age and may be associated with clinically significant morbidity. We studied the association between sleep-disordered breathing (SDB) with nocturnal atrial fibrillation or flutter (AF) and complex ventricular ectopy (CVE) in older men.
Methods: A total of 2911 participants in the Outcomes of Sleep Disorders in Older Men Study underwent unattended polysomnography. Nocturnal AF and CVE were ascertained by electrocardiogram-specific analysis of the polysomnographic data. Exposures were (1) SDB defined by respiratory disturbance index (RDI) quartile (a major index including all apneas and hypopneas), and ancillary definitions incorporating (2) obstructive events, obstructive sleep apnea (OSA; Obstructive Apnea Hypopnea Index quartile), or (3) central events, central sleep apnea (CSA; Central Apnea Index category), and (4) hypoxia (percentage of sleep time with <90% arterial oxygen percent saturation). Multivariable logistic regression analyses were performed.
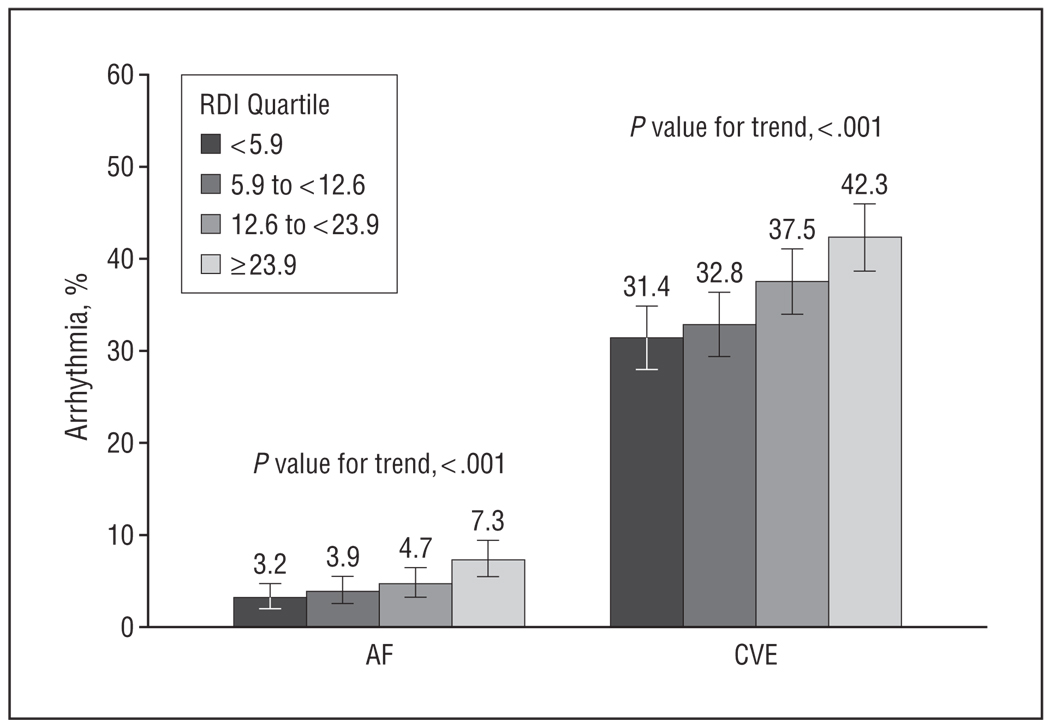
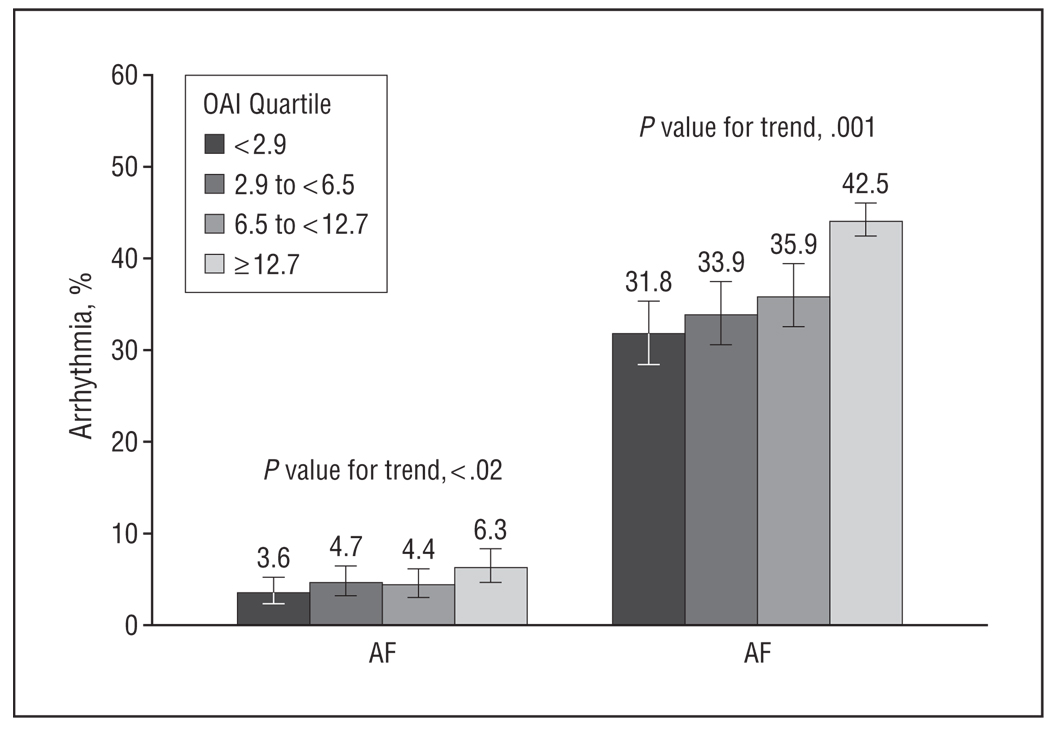
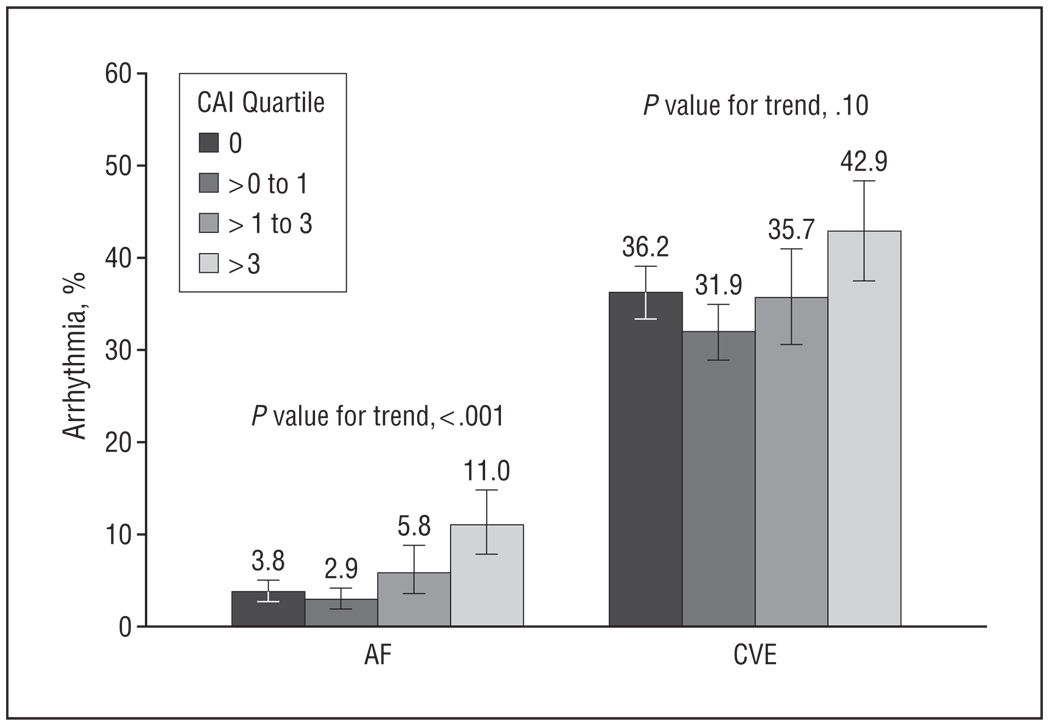
Results: An increasing RDI quartile was associated with increased odds of AF and CVE (P values for trend, .01 and <.001, respectively). The highest RDI quartile was associated with increased odds of AF (odds ratio [OR], 2.15; 95% confidence interval [CI], 1.19-3.89) and CVE (OR, 1.43; 95% CI, 1.12-1.82) compared with the lowest quartile. An increasing OSA quartile was significantly associated with increasing CVE (P value for trend, .01) but not AF. Central sleep apnea was more strongly associated with AF (OR, 2.69; 95% CI, 1.61-4.47) than CVE (OR, 1.27; 95% CI, 0.97-1.66). Hypoxia level was associated with CVE (P value for trend, <.001); those in the highest hypoxia category had an increased odds of CVE (OR, 1.62; 95% CI, 1.23-2.14) compared with the lowest quartile.
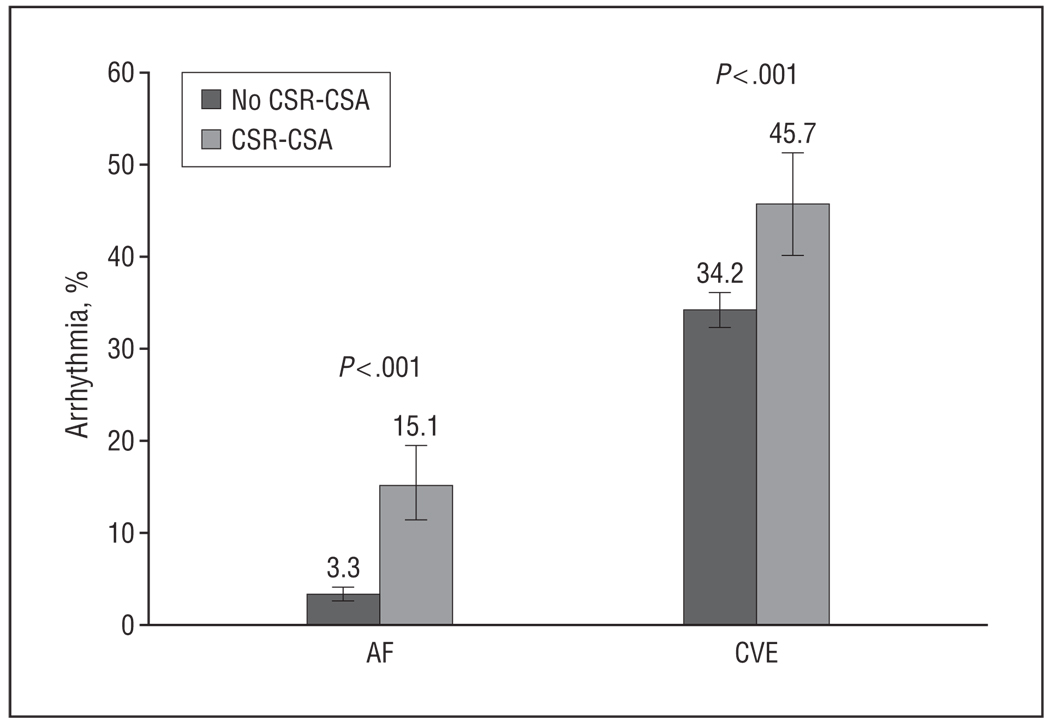
Conclusions: In this large cohort of older men, increasing severity of SDB was associated with a progressive increase in odds of AF and CVE. When SDB was characterized according to central or obstructive subtypes, CVE was associated most strongly with OSA and hypoxia, whereas AF was most strongly associated with CSA, suggesting that different sleep-related stresses may contribute to atrial and ventricular arrhythmogenesis in older men.
Figures
References
-
- Somers VK, Dyken ME, Skinner JL. Autonomic and hemodynamic responses and interactions during the Mueller maneuver in humans. J Auton Nerv Syst. 1993;44(2–3):253–259. - PubMed
-
- Arias MA, Alonso-Fernandez A, Garcia-Rio F, Sanchez A, Lopez JM, Pagola C. Obstructive sleep apnea in atrial fibrillation patients. Int J Cardiol. 2006;110(3):426. - PubMed
-
- Arias MA, Sanchez AM. Obstructive sleep apnea and its relationship to cardiac arrhythmias. J Cardiovasc Electrophysiol. 2007;18(9):1006–1014. - PubMed
-
- Flemons WW, Remmers JE, Gillis AM. Sleep apnea and cardiac arrhythmias: is there a relationship? Am Rev Respir Dis. 1993;148(3):618–621. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 AR45632/AR/NIAMS NIH HHS/United States
- R01HL070837/HL/NHLBI NIH HHS/United States
- R01 HL071194/HL/NHLBI NIH HHS/United States
- U01 AR45647/AR/NIAMS NIH HHS/United States
- R01 HL070842/HL/NHLBI NIH HHS/United States
- U01 AR045654/AR/NIAMS NIH HHS/United States
- U01AR45614/AR/NIAMS NIH HHS/United States
- U01-AG027810/AG/NIA NIH HHS/United States
- R01 HL070838/HL/NHLBI NIH HHS/United States
- U01 AR45583/AR/NIAMS NIH HHS/United States
- R01 HL070839/HL/NHLBI NIH HHS/United States
- R01 HL070837/HL/NHLBI NIH HHS/United States
- K23 HL079114/HL/NHLBI NIH HHS/United States
- R01 HL070848/HL/NHLBI NIH HHS/United States
- UL1RR024140/RR/NCRR NIH HHS/United States
- R01 HL070847/HL/NHLBI NIH HHS/United States
- U01 AR045614/AR/NIAMS NIH HHS/United States
- U01 AR45654/AR/NIAMS NIH HHS/United States
- U01 AR045583/AR/NIAMS NIH HHS/United States
- R01 HL070841/HL/NHLBI NIH HHS/United States
- U01 AR045647/AR/NIAMS NIH HHS/United States
- U01 AR45580/AR/NIAMS NIH HHS/United States
- U01 AG027810/AG/NIA NIH HHS/United States
- UL1 RR024140/RR/NCRR NIH HHS/United States
- U01 AR045580/AR/NIAMS NIH HHS/United States
- U01 AG18197/AG/NIA NIH HHS/United States
- U01 AG018197/AG/NIA NIH HHS/United States
- U01 AR066160/AR/NIAMS NIH HHS/United States
- U01 AR045632/AR/NIAMS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
