

Factors associated with peripartum hysterectomy
- PMID: 19546767
- PMCID: PMC2714706
- DOI: 10.1097/AOG.0b013e3181a81cdd
Factors associated with peripartum hysterectomy
Abstract
Objective: To identify factors associated with peripartum hysterectomy performed within 30 days postpartum.
Methods: This was a population-based case-control study using Washington State birth certificate registry (1987-2006) linked to the Comprehensive Hospital Abstract Reporting System. Cases underwent hysterectomy within 30 days postpartum. Controls were frequency matched 4:1. Exposures included factors related to hemorrhage, delivery method, multiple gestations, and infection. Incidence rates of peripartum hysterectomy and maternal and neonatal morbidity and mortality were assessed. Adjusted odds ratios (aORs) by maternal age, parity, gestational age, year of birth, and mode of delivery and 95% confidence intervals (CIs) were computed.
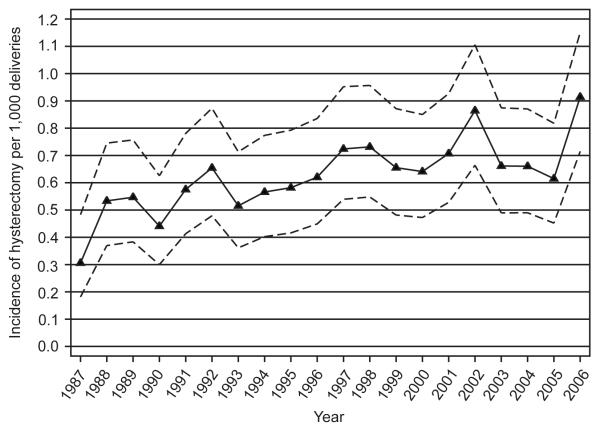
Results: There were 896 hysterectomies. Incidence rates ranged from 0.25 in 1987 to 0.82 per 1,000 deliveries in 2006 (chi for trend, P<.001). Factors related to hemorrhage were strongly related to peripartum hysterectomy. Placenta previa (192 cases compared with 23 controls; aOR 7.9, 95% CI 4.1-15.0), abruptio placenta (71 compared with 55; aOR 3.2, 95% CI 1.8-5.8), and retained placenta (214 compared with 28; aOR 43.0, 95% CI 19.0-97.7) increased the risk of hysterectomy, as did uterine atony, uterine rupture, and thrombocytopenia. Having multiple gestations did not. As compared with vaginal delivery, vaginal delivery after cesarean (27 cases compared with 105 controls; aOR 1.9, 95% CI 1.2-3.0), primary cesarean (270 compared with 504; aOR 4.6, 95% CI 3.5-6.0), and repeat cesarean (296 compared with 231; aOR 7.9, 95% CI 5.8-10.7) increased the risk of peripartum hysterectomy. Among the 111 women who had hysterectomy on readmission (12.8% of cases), hemorrhage- and infection-related factors were still strongly associated with peripartum hysterectomy.
Conclusion: Incidence rates of peripartum hysterectomy are increasing over time. The most important risk factor for peripartum hysterectomy is hemorrhage, most notably caused by uterine rupture, retained placenta, and atony of uterus.
Level of evidence: II.
Figures
Comment in
-
Factors associated with peripartum hysterectomy.Obstet Gynecol. 2009 Oct;114(4):927. doi: 10.1097/AOG.0b013e3181ba0383. Obstet Gynecol. 2009. PMID: 19888055 No abstract available.
References
-
- Briery CM, Rose CH, Hudson WT, et al. Planned vs emergent cesarean hysterectomy. Am J Obstet Gynecol. 2007;197:154.e1–154.e5. - PubMed
-
- Knight M. Peripartum hysterectomy in the UK: management and outcomes of the associated haemorrhage. BJOG. 2007;114:1380–1387. - PubMed
-
- Engelsen IB, Albrechtsen S, Iversen OE. Peripartum hysterectomy-incidence and maternal morbidity. Acta Obstet Gynecol Scand. 2001;80:409–412. - PubMed
-
- Selo-Ojeme DO, Bhattacharjee P, Izuwa-Njoku NF, Kadir RA. Emergency peripartum hysterectomy in a tertiary London hospital. Arch Gynecol Obstet. 2005;271:154–159. - PubMed
-
- Forna F, Miles AM, Jamieson DJ. Emergency peripartum hysterectomy: a comparison of cesarean and postpartum hysterectomy. Am J Obstet Gynecol. 2004;190:1440–1444. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
