

The diagnosis and treatment of primary hyperaldosteronism in Germany: results on 555 patients from the German Conn Registry
- PMID: 19547646
- PMCID: PMC2689591
- DOI: 10.3238/arztebl.2009.0305
The diagnosis and treatment of primary hyperaldosteronism in Germany: results on 555 patients from the German Conn Registry
Abstract
Background: Primary hyperaldosteronism (Conn's syndrome) is being diagnosed increasingly often. As many as 12% of patients with hypertension have the characteristic laboratory constellation of Conn's syndrome. Its diagnosis and treatment have not been standardized.
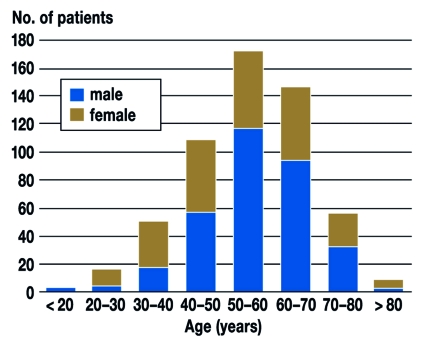
Methods: The authors retrospectively analyzed data of 555 patients (327 men and 228 women, aged 55 +/- 13 years) who were treated for primary hyperaldosteronism in 5 different centers from 1990 to 2006. The objective was to determine center-specific features of diagnosis and treatment.
Results: 353 (63%) of the patients had the hypokalemic variant of primary hyperaldosteronism; 202 never had documented hypokalemia. The centers differed markedly with respect to the patients' clinical presentation, diagnostic testing of endocrine function, and diagnostic imaging techniques, including adrenal venous sampling. The adrenalectomy rate ranged from 15% to 46%.
Conclusions: The registry data reveal an unexpected heterogeneity in the diagnostic evaluation and treatment of primary hyperaldosteronism. National or international guidelines are needed so that these can be standardized.
Keywords: Conn’s syndrome; aldosterone; hyperaldosteronism; hypertension; hypokalemia.
Figures




Comment in
-
Doubts.Dtsch Arztebl Int. 2009 Oct;106(42):692; author reply 692. doi: 10.3238/arztebl.2009.0692a. Epub 2009 Oct 16. Dtsch Arztebl Int. 2009. PMID: 19946439 Free PMC article. No abstract available.
References
-
- Fardella C, Mosso L, Gómez-Sánchez C, Cortés P, Soto J, Gómez L, et al. Primary aldosteronism in essential hypertensives: prevalence, biochemical profile, and molecular biology. J Clin Endocrinol Metab. 2000;85:1863–1867. - PubMed
-
- Mulatero P, Dluhy R, Giacchetti G, Boscaro M, Veglio F, Stewart P. Diagnosis of primary aldosteronism: from screening to subtype differentiation. Trends in Endocrinology and Metabolism. 2005;16:114–119. - PubMed
-
- Loh K, Koay E, Khaw M, Emmanuel S, Young W. Prevalence of primary aldosteronism among Asian hypertensive patients in Singapore. J Clin Endocrinol Metab. 2000;85:2854–2859. - PubMed
-
- Fogari R, Preti P, Zoppi A, Rinaldi A, Fogari E, Mugellini A. Prevalence of primary aldosteronism among unselected hypertensive patients: a prospective study based on the use of an aldosterone/renin ratio above 25 as a screening test. Hypertens Res. 2007;30:111–117. - PubMed
-
- Wolf-Maier K, Cooper R, Banegas J, Giampaoli S, Hense H, Joffres M, et al. Hypertension prevalence and blood pressure levels in 6 European countries, Canada, and the United States. JAMA. 2003;289:2363–2369. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials