

Coinfection with HIV-1 and HCV--a one-two punch
- PMID: 19549523
- PMCID: PMC3146750
- DOI: 10.1053/j.gastro.2009.06.040
Coinfection with HIV-1 and HCV--a one-two punch
Abstract
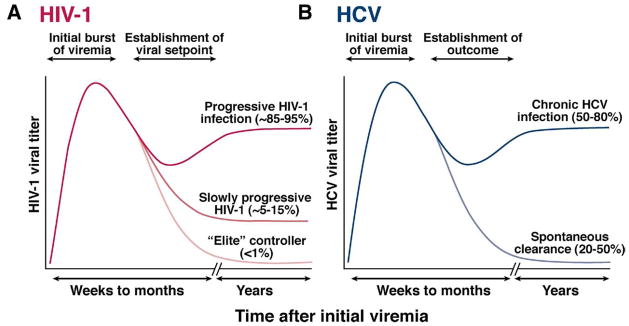
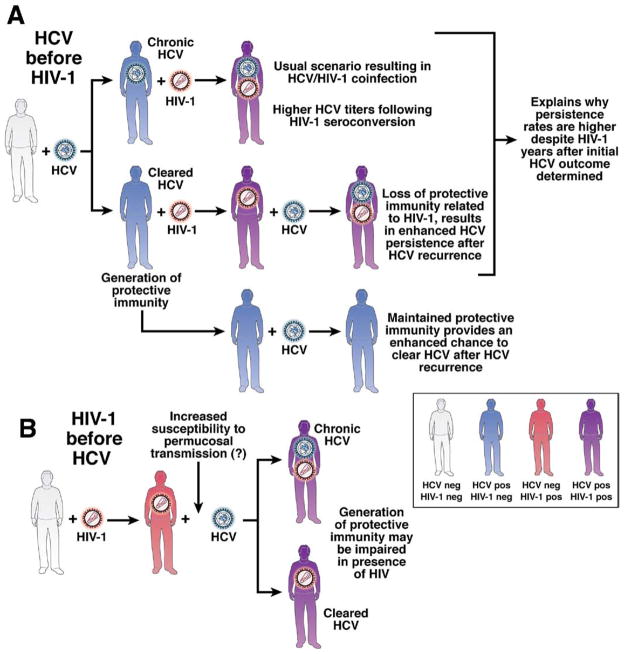
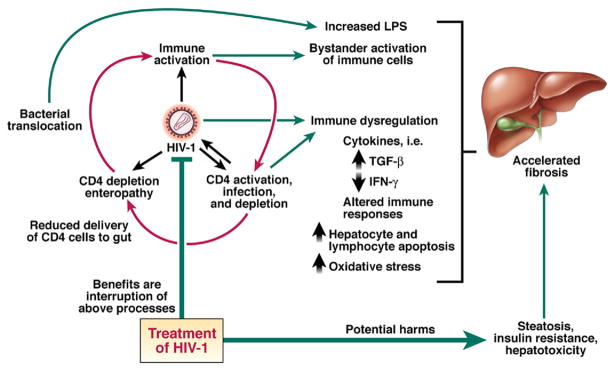
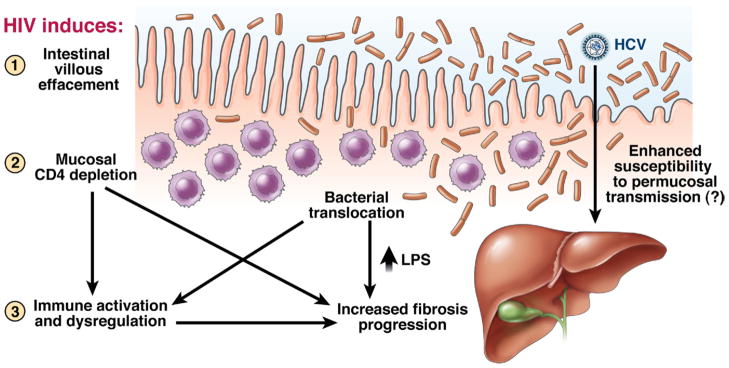
Hepatitis C virus (HCV) infection is a major cause of chronic liver disease, cirrhosis, and death; it is estimated that 180 million persons are infected with HCV worldwide. The consequences of HCV are worse in those who are coinfected with human immunodeficiency virus 1 (HIV-1), which is unfortunately a common scenario because of shared risk factors of the viruses. More studies into effects of HCV/HIV-1 coinfection are needed, but efforts have been hampered by limitations in our understanding of the combined pathogenesis of the 2 viruses. Gaining insight into the mechanisms that underlie the immunopathogenesis of these persistent viral infections could lead to new therapeutic strategies for patients with HCV/HIV-1 coinfection.
Conflict of interest statement
Conflicts of interest
The authors disclose the following: R.T.C. receives research grant support from Roche Labs and Schering-Plough. A.Y.K. discloses no conflicts.
Figures
References
-
- Sulkowski MS, Thomas DL. Hepatitis C in the HIV-infected person. Ann Intern Med. 2003;138:197–207. - PubMed
-
- Deeks SG, Walker BD. Human immunodeficiency virus controllers: mechanisms of durable virus control in the absence of antiretroviral therapy. Immunity. 2007;27:406–416. - PubMed
-
- Maheshwari A, Ray S, Thuluvath PJ. Acute hepatitis C. Lancet. 2008;372:321–332. - PubMed
-
- Jauncey M, Micallef JM, Gilmour S, et al. Clearance of hepatitis C virus after newly acquired infection in injection drug users. J Infect Dis. 2004;190:1270–1274. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
